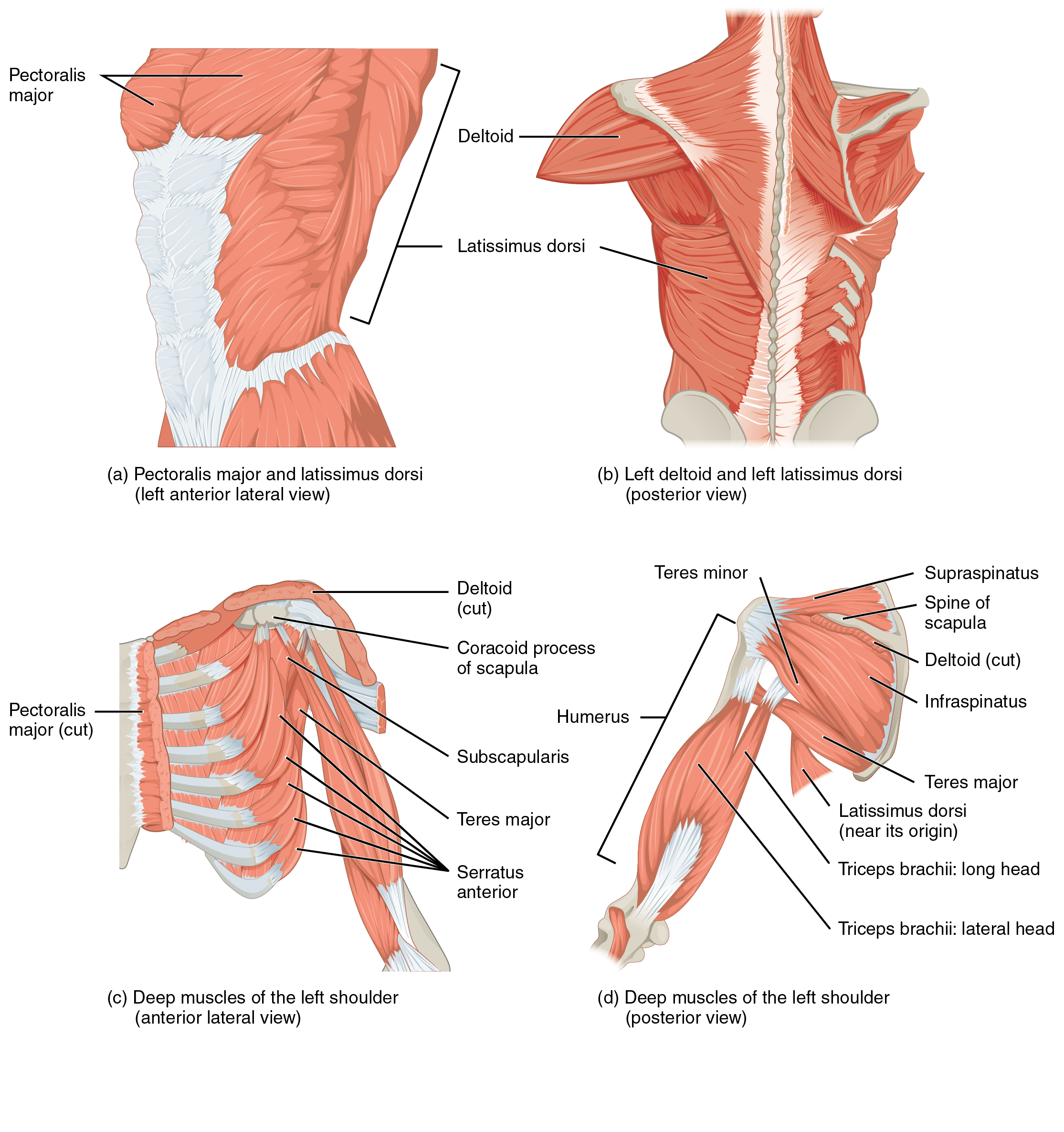
Subscapularis Muscle
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Subscapularis | Subscapular fossa | Lesser tubercle of Humerus | Upper Subscapular n. Lower Subscapular n. C5 - C6 |
GHJ: IR, Stabilization |
Origin
Insertion
Innervation
Action
GHJ: Internal Rotation, Adduction6
Test
- Lift-off Test (Gerber’s test)
- Bear hug test
- Belly press test (Napolean Test)
- “performed by having the patient place the affected hand on the abdomen and attempt to move the elbow anteriorly. The test was considered positive if the patient could not move the elbow forward”gillPhysicalExaminationPartial2007?
Release
- Patient in supine
- Stand on the patient’s ipsilateral side, facing the patient.
- squeeze the patient’s forearm with your elbow against your side and hold their arm with your hand.
- With the other hand, palpate the lateral border of the scapula
- Move to the superior 2/3 or halfway up the scapula
- Keep your wrists pronated so your fingertips are against the anterior aspect of the scapula
- Drive medially on the anterior scapula
- Once you have moved far enough medially, IR your shoulder and drive your fingertips perpendicular to the scapula to push into the subscapularis muscle
Note
Sometimes patients can feel neurological symptoms of pain radiating up to the neck or down to the arm. This is common due to the relationship of the subscapularis tissue and the nearby neurovasculature
Strain-Counterstrain
References
1.
Betts JG, Blaker W. Openstax Anatomy and Physiology. 2nd ed. OpenStax; 2022. https://openstax.org/details/books/anatomy-and-physiology-2e/?Book%20details
2.
Gray H. Anatomy of the Human Body. 20th ed. (Lewis WH, ed.). Lea & Febiger; 1918. https://www.bartleby.com/107/
3.
Donnelly JM, Simons DG, eds. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual. Third edition. Wolters Kluwer Health; 2019.
4.
Neumann DA, Kelly ER, Kiefer CL, Martens K, Grosz CM. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 3rd ed. Elsevier; 2017.
5.
Weinstock D. NeuroKinetic Therapy: An Innovative Approach to Manual Muscle Testing. North Atlantic Books; 2010.
6.
Gilroy AM, MacPherson BR, Wikenheiser JC, Voll MM, Wesker K, Schünke M, eds. Atlas of Anatomy. 4th ed. Thieme; 2020.
7.
Myers HL, Devine WH, Fossum C, et al. Compendium Edition: Clinical Application of Counterstrain. Compendium ed. Osteopathic Press; 2012.
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Subscapularis Muscle.
https://yomokerst.com/The
Archive/Anatomy/Skeletal Muscles/Upper Limb Muscles/Intrinsic Shoulder
Muscles/Rotator Cuff/subscapularis.html