Biceps Brachii
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Biceps brachii Long head | Supraglenoid tubercle of scapula Adjacent rim of Glenoid Labrum |
Radial tuberosity Bicipital aponeurosis |
Musculocutaneous n. C5 - C6 |
Elbow: Flexion, Supination GHJ: Flexion, Stabilization of humeral head during deltoid contraction, Abduction, IR |
| Biceps brachii Short head | Coracoid process | Radial tuberosity Bicipital aponeurosis |
Musculocutaneous n. C5 - C6 |
Elbow: Flexion, Supination GHJ: Flexion, Stabilization of humeral head during deltoid contraction, Abduction, IR |
Origin
The long head of the biceps inserts superiorly to the glenoid on:
The short head of the biceps inserts anterior to the glenoid on:
- Coracoid process of Scapula5
Insertion
Both heads of the biceps share a common insertion:
Innervation
Action
- Shoulder: Flexion
- GHJ: Abduction, Internal rotation, Stabilization of humeral head during deltoid contraction5
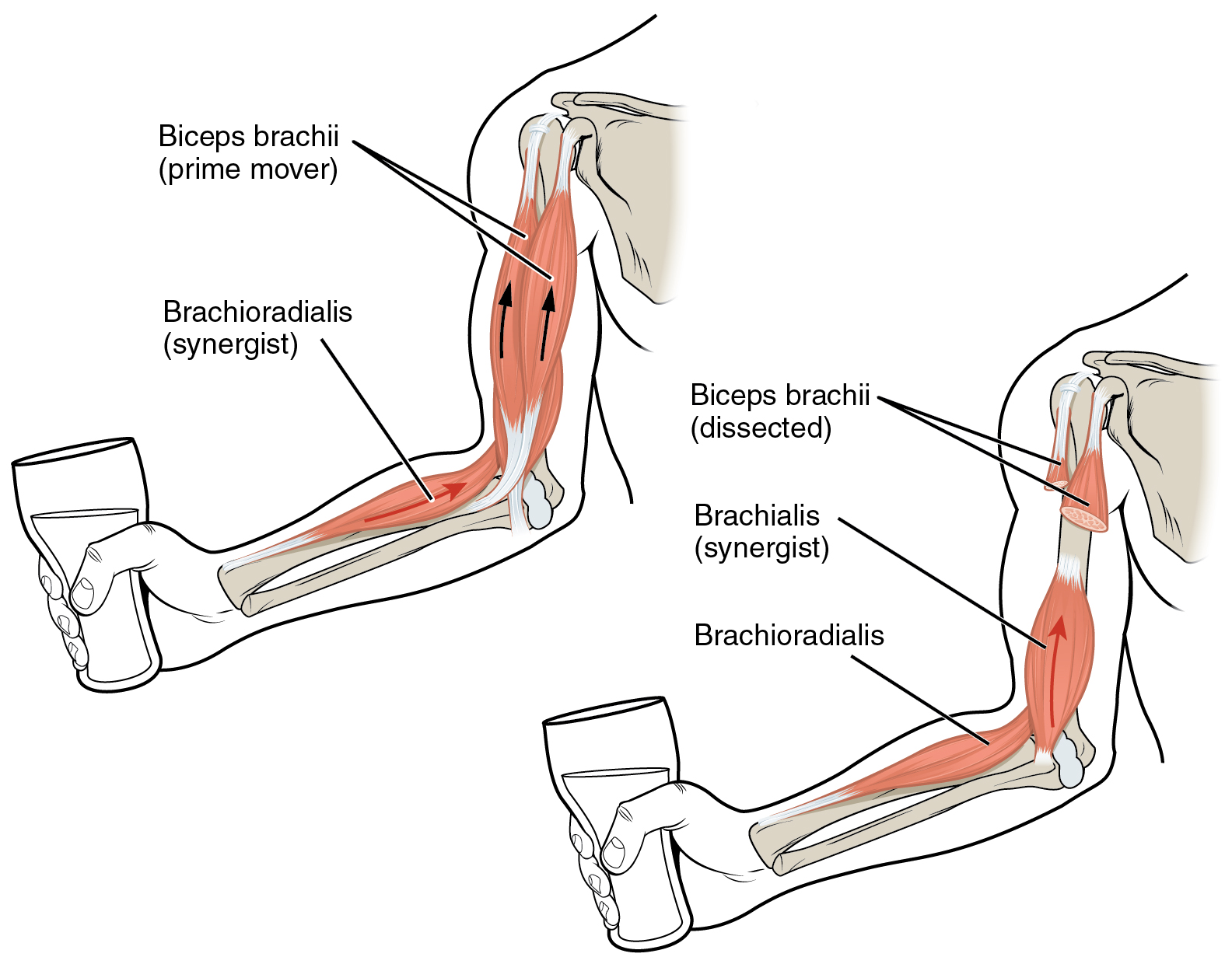
- Elbow: Flexion; Supination5
The biceps are most efficient at supination when the elbow is flexed to 90°7.
Biceps contraction places the radius at an increased chance of anterior and proximal dislocation, but this is prevented due to the annular ligament7.
The biceps brachii long head is also involved in abduction and a rupture will result in ~20% decrease in abduction strength7.
How does the Biceps Brachii Long head function as a GHJ stabilizer?
“When the elbow is flexed, the biceps brachii acts as a powerful supinator because the lever arm is almost perpendicular to the axis of pronation/supination.”5
Note: When the elbow is flexed, the biceps brachii acts as a powerful supinator because the lever arm is almost perpendicular to the axis of pronation/supination.5
Anatomy
Tendon
The tendon of the Long Head of the Biceps Brachii “…crosses over the humeral head as it courses distally toward the intertubercular groove on the anterior humerus”3
Clinical Relevance
The biceps may have a role in GHJ stabilization9
Dysfunction
Biceps dysfunction is difficult to diagnose “One confounding factor is that there is no known pain pattern specific for the biceps tendon. Although biceps tendon pain can radiate down the front of the shoulder, pain into the front of the shoulder can be secondary to a variety of causes, including rotator cuff injury”gillPhysicalExaminationPartial2007?
Palpation
Tenderness to Palpation
- signs of biceps tendon injury.
- Eliciting point tenderness by palpation of the biceps tendon in the biceps groove 3 to 6 cm below the anterior acromion with the arm in approximately 10° of internal rotationgillPhysicalExaminationPartial2007?
- area of point tenderness should move as the arm rotates internally and externallgillPhysicalExaminationPartial2007?
- Positive test: “pain elicited in the bicipital groove to deep pressure in the involved shoulder compared with no pain elicited with similar pressure to the bicipital groove of the opposite shoulder”gillPhysicalExaminationPartial2007?
- “Overall, tenderness on palpation had a sensitivity of 53%, a specificity of 54%, an accuracy of 54%, and a likelihood ratio of 1.13”gillPhysicalExaminationPartial2007?
Tests
- Speed’s Test
- Palpation
- Speeds + Biceps palpation
- “If the patient had a positive Speed’s test and pain with biceps palpation, the combined positive tests yielded a sensitivity of 68%, a specificity of 49%, an accuracy of 59%, and a likelihood ratio of 1.31”gillPhysicalExaminationPartial2007?
“Two commonly used techniques for making the diagnosis of biceps tendinitis are Speed’s test and palpation that elicits tenderness over the bicipital groove.”gillPhysicalExaminationPartial2007?
Special Test
Speed’s Test
- Patient standing with the elbow extended and the forearm in supination, the arm was elevated to 90° and extended slightly horizontallygillPhysicalExaminationPartial2007?
- Pt resists the downward force applied by the examiner10
- Positive: Pain was localized to the bicipital groove area in the anterior shoulder10
Possible tests for biceps injury
- Some researchers suggest that the lift-off test can be positive for pts with biceps tendon injurygillPhysicalExaminationPartial2007?
- Theorizing that attempting to lift the affected arm off the back might provoke pain or weakness secondary to biceps tendon teargillPhysicalExaminationPartial2007?
“Only the lift-off test and the belly press test had a likelihood ratio of more than 2.0. These 2 tests had low sensitivities (0.28 and 0.17, respectively) but high specificity (0.89 and 0.92, respectively)”10