Musculocutaneous nerve

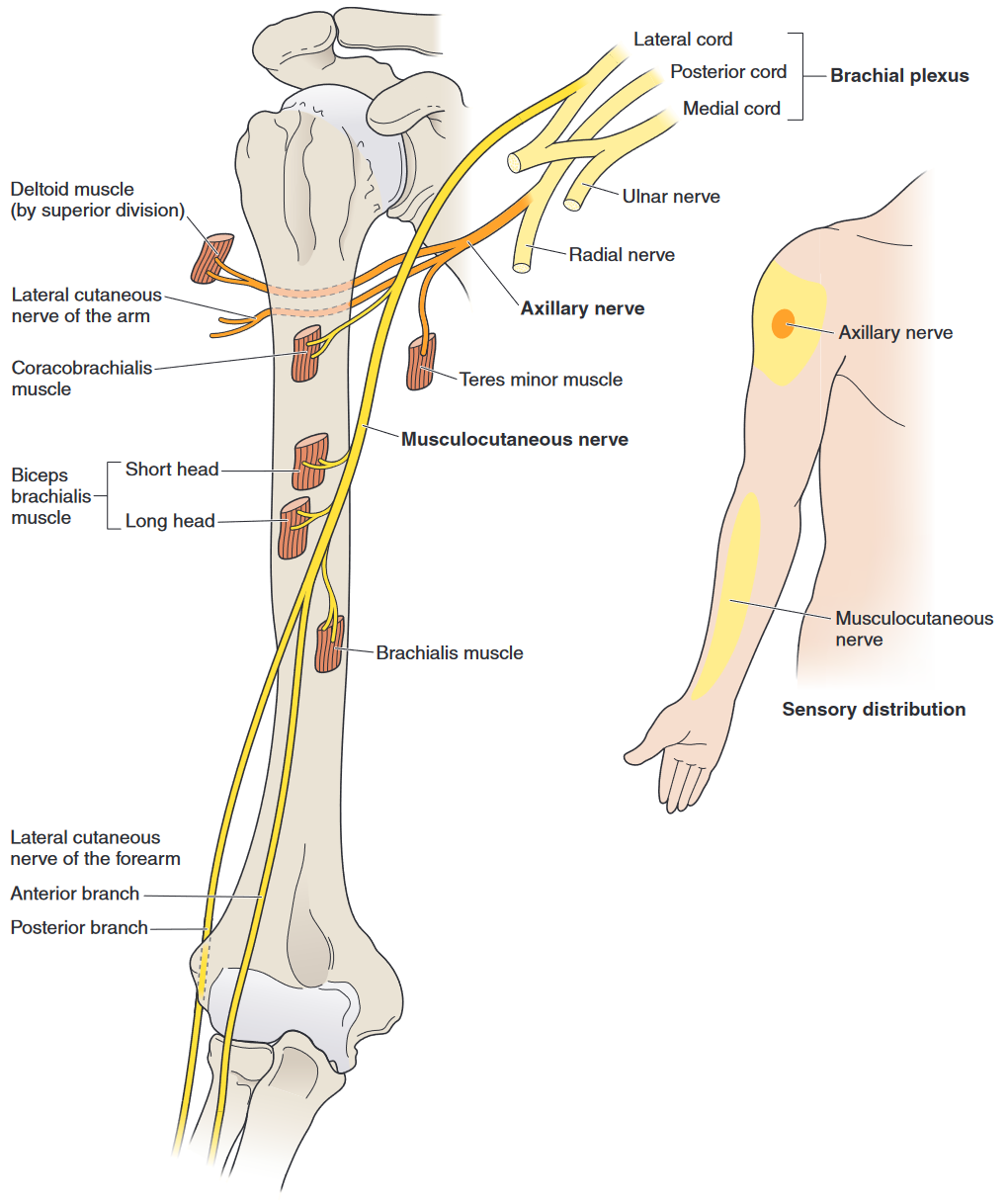
The musculocutaneous nerve (Fig. 3-10) is the terminal branch of the lateral cord, which in turn is derived from the anterior division of the upper and middle trunks of the fifth through seventh cervical nerve roots.1
Anatomy
Origin
The musculocutaneous nerve arises from the terminal branch of the lateral cord which comes from anterior divisions of the Superior trunk and middle trunk and thus is supplied by nerve roots C5, C6, C71.
 nerve.png)
Path
After arising from the lateral cord of the brachial plexus at the level of coracoid process and proceeds caudally and laterally1. As it travels caudally and laterally down the arm, the musculocutaneous nerve gives branches to the coracobrachialis, before penetrating this muscle 3–8 cm below the coracoid process1. The nerve then runs through and supplies, the biceps brachii and partially innervates brachialis muscles, before emerging between the biceps brachii and the brachioradialis muscles 2–5 cm above the elbow1. After emerging between the biceps and brachioradialis (2-5cm above the elbow), the musculocutaneous nerve becomes the Lateral Cutaneous (antebrachial) Nerve of the Forearm which supplies the anterior-lateral aspect of the forearm1.
Innervation
Motor innervation
Cutaneous Innervation
The Musculocutaneous nerve becomes the
Dysfunction
- Coracobrachialis entrapment1
Lesion
- Muscular impact Coracobrachialis, biceps brachii, and brachialis
- Impact: Weak elbow flexion with forearm supinated1
Etiology
Atraumatic
Cases of atraumatic isolated musculocutaneous neuropathies are rare1. Reported cases include poor positioning while under anesthesia, neoplastic structures impinging the musculocutaneous nerve, and strenuous upper extremity exercise without apparent underlying disease1. Some theorize that exercise-related cases are caused by entrapment of the nerve within the coracobrachialis and/or traction between a proximal fixation point at the coracobrachialis and a distal fixation point at the deep fascia at the elbow1.
Injury to this nerve can also result from demanding physical work involving shoulder flexion and repetitive elbow flexion with a pronated forearm.35 Although rare, an isolated lesion to the musculocutaneous nerve can result in weakness of the biceps, coracobrachialis, and brachialis (Table 3-3). These muscles help stabilize the elbow and the G-H joint and maintain the static position of the arm.
Clinical Presentation
The typical clinical presentation includes ▶ reports or evidence of muscle wasting and sensory changes to the lateral side of the forearm; ▶ weakness of the biceps, brachialis, and coracobrachialis; ▶ diminished biceps reflex; ▶ decreased sensation at the lateral forearm; and ▶ positive electromyogram (EMG) study.
Examination
Intervention
Conservative Intervention
Conservative intervention as recommended by Dutton incldues cessation of aggravating activities and a gradual return to activity with resolution of symptoms1.
References
1.
Dutton M. Dutton’s Orthopaedic Examination, Evaluation, and Intervention. 5th ed. McGraw Hill Education; 2020.
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Musculocutaneous nerve.
https://yomokerst.com/The
Archive/Anatomy/Nerves/Upper extremity
nerves/musculocutaneous_nerve.html