Gluteus Minimus Muscle
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Gluteus Minimus | Ilium gluteal surface (inferior to gluteus medius origin) | Greater trochanter (anterolateral surface) | Superior gluteal n. L4 - S1 |
Entire mm.: Abduction, Frontal stabilization Anterior fibers: Flexion, IR Posterior fibers: Extension, ER (when <60° HF), IR (when >60° HF) |
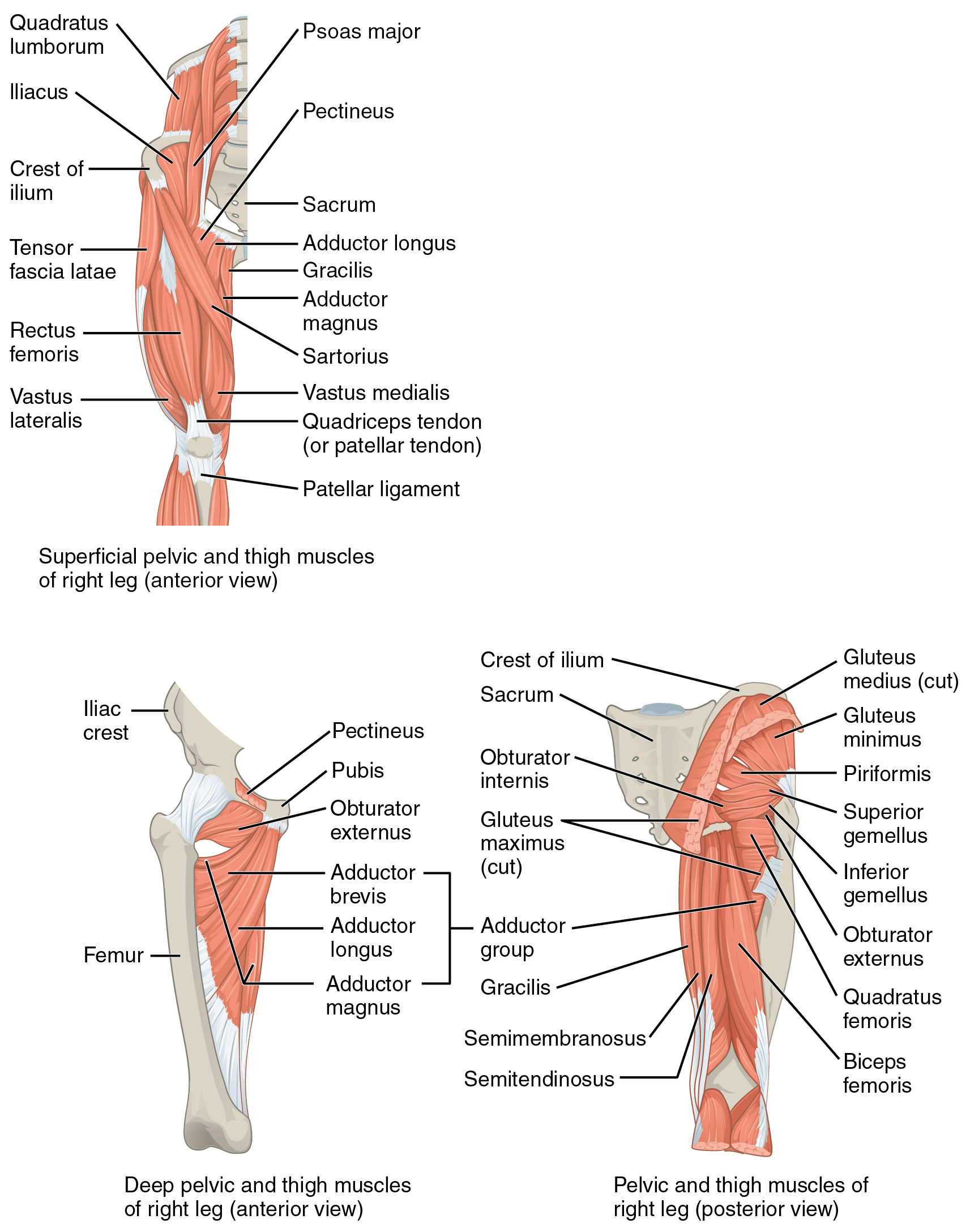
Origin
Ilium (gluteal surface below the origin of gluteus medius)6
Insertion
Greater trochanter of the femur (anterolateral surface)6
Innervation
The gluteus maximus muscle is innervated by nerve roots L4, L5, and S1, via the Superior gluteal nerve6
Action
- Entire muscle: abducts the hip, stabilizes the pelvis in the coronal plane6
- Anterior fibers: flexion and internal rotation6
- Posterior fibers: extension and external rotation6
At ≥60° hip flexion, the posterior fibers of the gluteus minimus switch and produce an internal rotation torque4.
The gluteus minimus generates a force equivalent of ~4.9kg, which is 3x less than the glute med7.
Palpation
- Position the patient in sidelying8
- Much of the glute medius and minimus overlap, but you can isolate the gluteus medius by palpating the most superior part of the iliac crest8.
- The glute med’s proximal origin extends from the PSIS almost to the ASIS8.
- The fibers of the glute med and min are fanned across the iliac crest then converge distally at the greater trochanter of the femur8.
- To palpate the gluteus minimus, dive deep to the the gluteus medius
- Having the patient actively abduct the top leg will help confirm that you are palpating the correct muscle8.
Pain Referral pattern
Exercises
A wedge forcing the foot into hyper-dorsiflexion will cause the client to prevent excessive anterior knee translation and force more hip hinge, which will activate the glutes.
- Single leg bridge (with 90° knee flexion and pushing through the hindfoot)
- Wall triple extension
- Bridge (toes up)
- S/L Hip abduction to high knee
References
1.
Betts JG, Blaker W. Openstax Anatomy and Physiology. 2nd ed. OpenStax; 2022. https://openstax.org/details/books/anatomy-and-physiology-2e/?Book%20details
2.
Gray H. Anatomy of the Human Body. 20th ed. (Lewis WH, ed.). Lea & Febiger; 1918. https://www.bartleby.com/107/
3.
Donnelly JM, Simons DG, eds. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual. Third edition. Wolters Kluwer Health; 2019.
4.
Neumann DA, Kelly ER, Kiefer CL, Martens K, Grosz CM. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 3rd ed. Elsevier; 2017.
5.
Weinstock D. NeuroKinetic Therapy: An Innovative Approach to Manual Muscle Testing. North Atlantic Books; 2010.
6.
Gilroy AM, MacPherson BR, Wikenheiser JC, Voll MM, Wesker K, Schünke M, eds. Atlas of Anatomy. 4th ed. Thieme; 2020.
7.
Jones B. B Project Foundations. b Project; 2025.
8.
Biel A. Trail Guide to the Body: A Hands-on Guide to Locating Muscles, Bones, and More. 6th ed. Books of Discovery; 2019.
9.
Myers HL, Devine WH, Fossum C, et al. Compendium Edition: Clinical Application of Counterstrain. Compendium ed. Osteopathic Press; 2012.
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Gluteus Minimus Muscle.
https://yomokerst.com/The
Archive/Anatomy/Skeletal Muscles/Lower limb muscles/Gluteal
Muscles/gluteus_minimus.html