Brachial Plexus

Anatomy
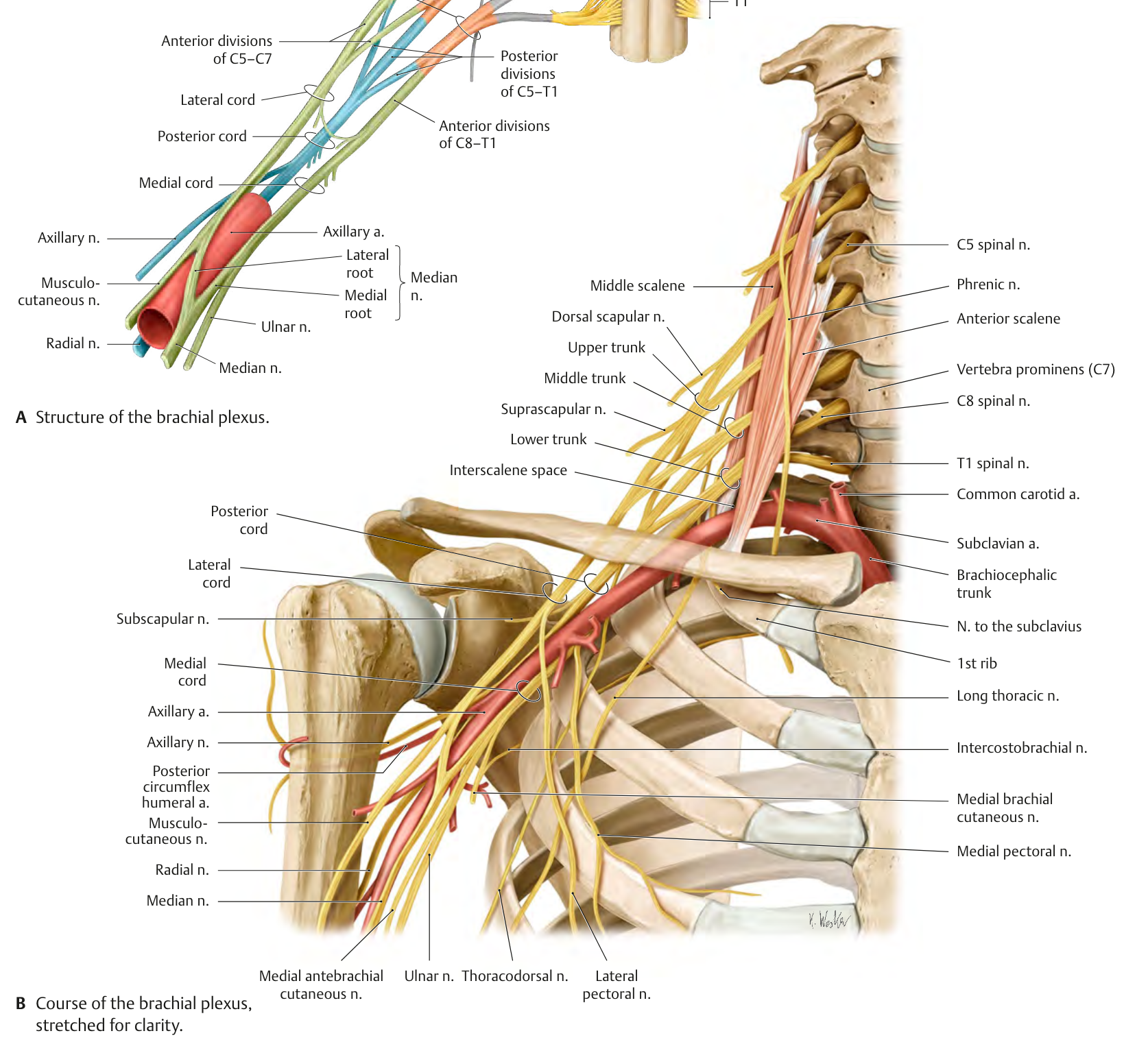
Nerve roots
The anterior divisions of 5 nerve roots compose the brachial plexus:
Trunks
The brachial plexus nerve roots become 3 trunks:
- Superior Trunk (C5, C6)2
- Middle Trunk (C7)2
- Inferior Trunk (C8, T1)2
Superior Trunk
- Nerve to Subclavius (C5, C6) originates from the Superior Trunk2
- The suprascapular nerve (C5, C6) originates from the Superior Trunk at Erb’s point2.
Divisions
6 divisions are formed from the 3 trunks:
- Anterior Division of the Superior Trunk
- Posterior Division of the Superior Trunk
- Anterior Division of the Middle Trunk
- Posterior Division of the Middle Trunk
- Anterior Division of the Inferior Trunk
- Posterior Division of the Inferior Trunk
Cords
The divisions then combine to form 3 cords:
- Lateral cord
- Posterior cord
- Medial cord
These three cords are named for their geographical relationship to the axillary artery2
The medial and lateral pectoral nerves extend from the medial and lateral cords, respectively (see Fig. 3-9). They supply the pectoralis major and pectoralis minor muscles. The pectoralis major muscle has dual innervation.1 The lateral pectoral nerve (C5–7), which is more medial in the muscle, travels with the thoracoacromial vessels, and innervates the clavicular and sternal heads. The medial pectoral nerve (C8–T1) shares a course with the lateral thoracic vessels and provides innervation to the sternal and costal heads.1 The main trunk of these nerves can be found near the origin of the vascular supply of the muscle.
The thoracodorsal nerve, or middle subscapular nerve, which arises from the posterior cord of the brachial plexus with its motor fiber contributions from C6, C7, and C8 (see Fig. 3-9). This nerve courses along the posterior–lateral chest wall, along the surface of the serratus anterior, and deep to the subscapularis, giving rise to branches that supply the latissimus dorsi. ■ The lower subscapular nerve (C5–6) to the teres major and part of the subscapularis muscle (see Fig. 3-9). ■ Sensory branches of the medial cord (C8–T1 or T1 alone) comprise the medial cutaneous (antebrachial) nerve to the medial surface of the forearm and the medial cutaneous (brachial) nerve to the medial surface of the arm (see Fig. 3-9).1
Lateral Cord
- Contributions to the Medial Pectoral Nerve (C8, T1)2
- Contributions to the Lateral Pectoral Nerve (C5, C6, C7)2
Posterior Cord
Medial Cord
Branches
- Musculocutaneous nerve (C5, C6, C7)
- Axillary nerve (C5, C6)
- Radial nerve (C5, C6, C7, C8, T1)
- Musculocutaneous nerve (C5, C6, C7)
- Musculocutaneous nerve (C5, C6, C7)
Traumatic Injury
Traumatic injuries to the brachial plexus typically involve a combination of different injuries:2
- Compression of spinal nerves2
- Traction injuries of spinal roots and nerves2
- Avulsions of spinal roots2
If the rootlets are disconnected from the spinal cord via trauma, they generally exit the intradural space, but in some rare cases they can remain in the space2
Obstetric Lesions
The main cause of brachial plexus injuries are due to difficulties during childbirth2.
Obstetric brachial plexus palsy is usually caused by stretch (neurapraxia or axonotmesis) and incomplete rupture more often than complete rupture or avulsion2.
“Klumpke’s paralysis is characterized by paralysis and atrophy of the small hand muscles and flexors of the wrist (the so-called claw-hand). Prognosis of this type is more favorable. If the sympathetic rami of T1 are involved, Horner syndrome (ptosis, enophthalmos, facial reddening, and anhydrosis) may be present.25”2
Dysfunction
Brachial Plexus irritation
Tests and measures
Release
This brachial plexus myofascial release technique was taught to me by Brad Jones4.
- Patient positioned in supine
- Stand on the patient’s ipsilateral side and face the patient’s head.
- Press into the axillary space and palpate the peripheral nerves running through the space to the upper extremity
- Pin the structures then bring the arm into abduction/elevation