Plantaris Muscle
Overview
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Plantaris | Lateral epicondyle of Femur | Calcaneal tuberosity | Tibial n. S1 - S2 |
Knee: *negligble* Flexion TCJ: PF Proprioception: Organ of proprioception for the plantarflexors |
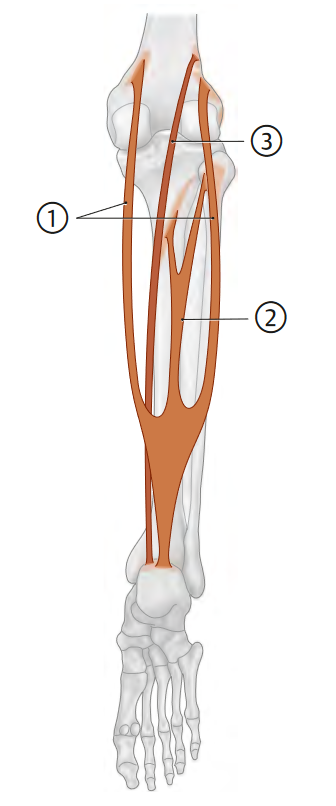
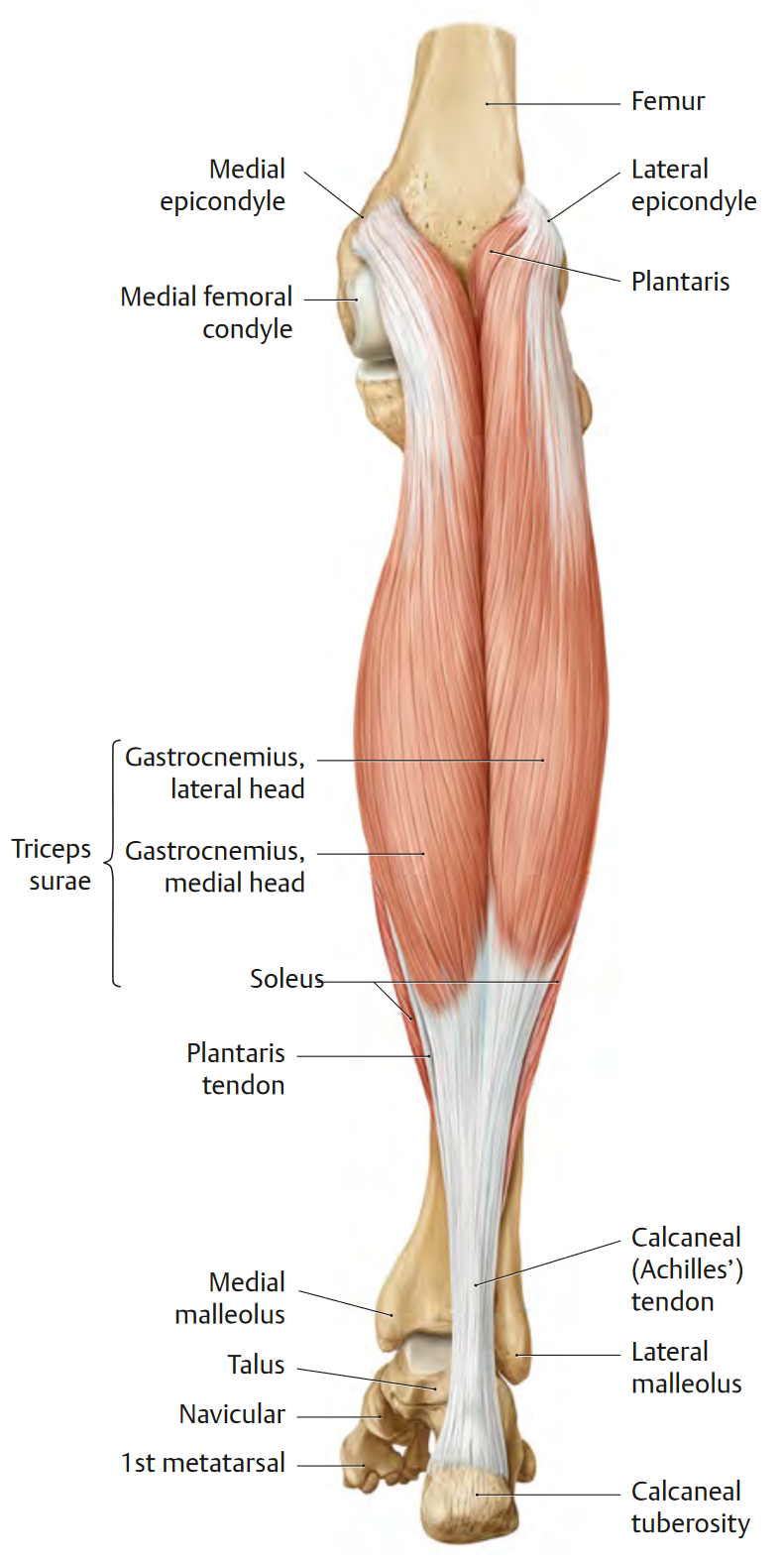
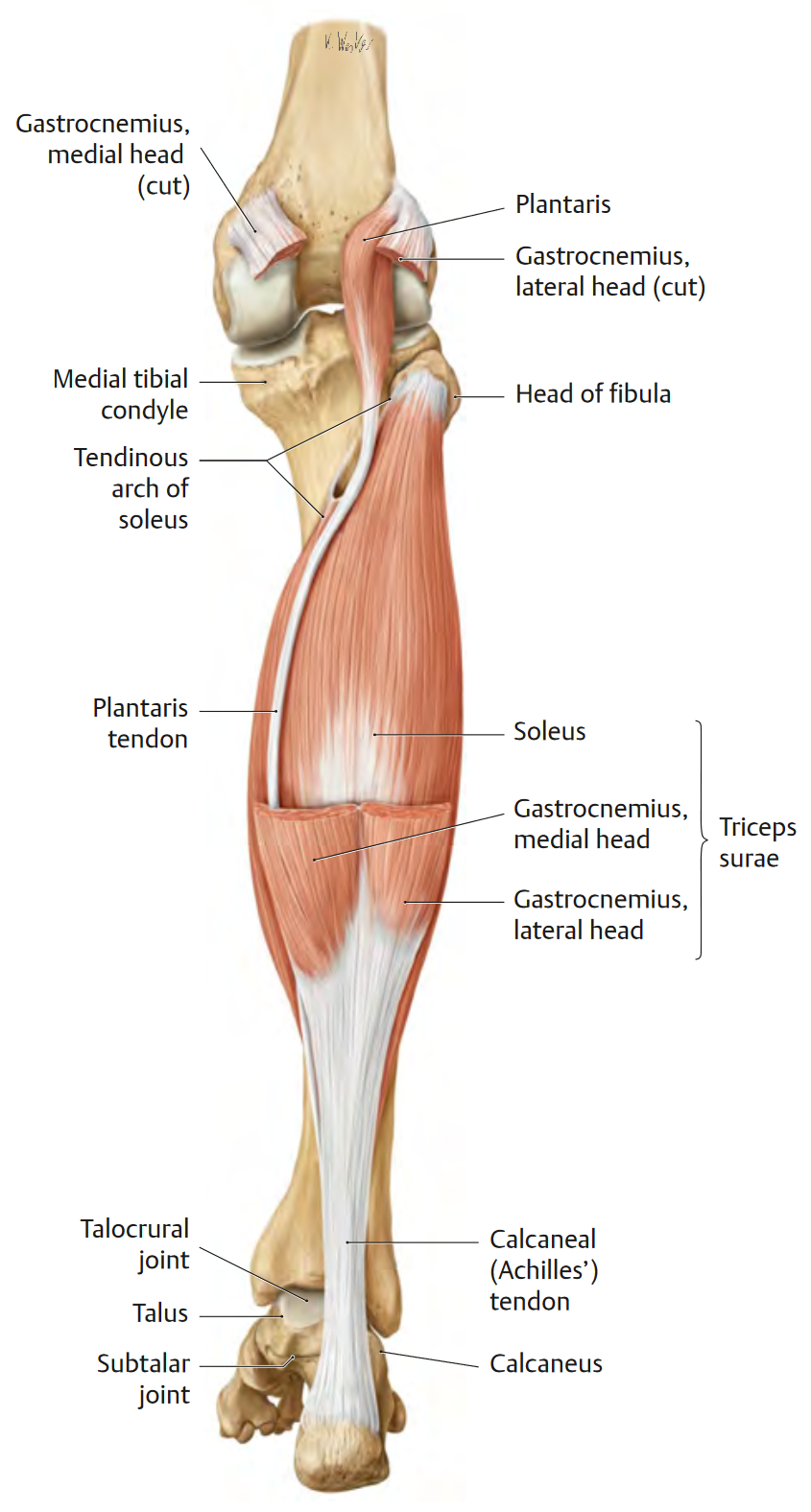
Origin
Lateral epicondyle of Femur (proximal to lateral head of gastrocnemius)1
Insertion
Calcaneal tuberosity1
Innervation
Action
Examination
Strength Test
- “Plantar flexion strength can be tested initially in non–weight-bearing (Fig. 21-22). However, unless there is significant weakness, clinician strength is usually insufficient to overcome ankle plantar flexor force, which necessitates a weight-bearing assessment of ankle plantar flexor strength. If no plantar flexion weakness is apparent in non–weight-bearing, a heel raise test is performed in the functional position, standing with the knee extended and the opposite foot off the floor Technically, one heel raise through full ROM, while standing with support on one leg, scores a 3/5 (fair) with manual muscle testing, with five single-limb heel raises scoring a 4/5 (good) and 10 single-limb heel raises scoring a 5/5 (normal). From a functional viewpoint, a wider range of scoring can sometimes prove more useful. Table 21-9 outlines an alternative scoring method. An alternative test, which is frequently used to assess talocrural and overall ankle function and is ften prescribed as an exercise, is the heel rise task. The task is performed using a block or a step, and the patient is positioned in standing with the balls of both feet on the block/step edge and the remaining parts of the feet over the edge. The patient may use a solid object for balance only. The patient is then asked to rise and lower his or herself on the balls of their feet as far as possible in each direction. The test can be also applied having the patient stand on only one leg. It is interesting to note that one study75 that measured both the ankle plantar flexion angle and the ankle dorsiflexion angle during this task found that the angles achieved were 23.7 degrees and 30.4 degrees respectively. The apparently large dorsiflexion angle compared to what is typically measured using a goniometer is likely the result that the motion combines both talocrural movement and forefoot movement.11 Although the task of raising up on the toes is generally thought to be predominantly performed by the triceps surae, a study by Kulig et al.76 reported significant contributions of the fibularis muscles and tibialis posterior during this task.”3
Pails & Rails
P.A.I.L.’s
- Plantarflexion
R.A.I.L.’s
- Dorsiflexion
Stretch
References
1.
Gilroy AM, MacPherson BR, Wikenheiser JC, Voll MM, Wesker K, Schünke M, eds. Atlas of Anatomy. 4th ed. Thieme; 2020.
2.
Spina AA. The plantaris muscle: Anatomy, injury, imaging, and treatment. The Journal of the Canadian Chiropractic Association. 2007;51(3):158-165.
3.
Dutton M. Dutton’s Orthopaedic Examination, Evaluation, and Intervention. 5th ed. McGraw Hill Education; 2020.
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Plantaris Muscle. https://yomokerst.com/The
Archive/Anatomy/Skeletal Muscles/Lower limb muscles/Knee and Lower
Leg/Posterior compartment/plantaris_muscle.html