Gluteus Medius
The Main Hip Abductor
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Gluteus medius | Ilium | Greater trochanter (lateral surface) | Superior gluteal n. L4 - S1 |
Entire mm.: Abduction, Frontal stabilization Anterior fibers: Flexion, IR Posterior fibers: Extension, ER (when <60° HF), IR (when >60° HF) |
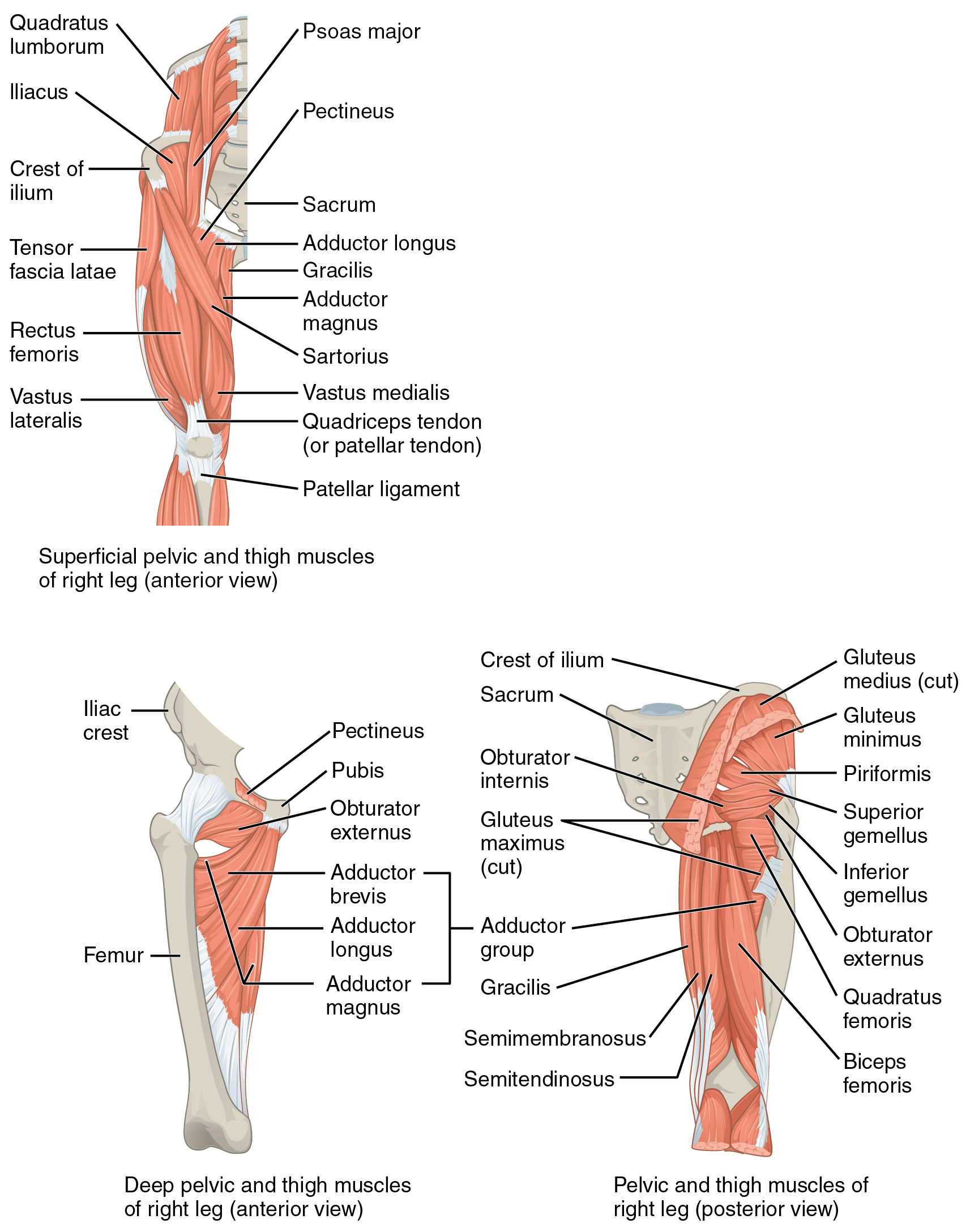
Origin
Ilium (gluteal surface below the iliac crest between the anterior and posterior gluteal line)6
Insertion
Greater trochanter of the femur (lateral surface)6
Innervation
The gluteus maximus muscle is innervated by nerve roots L4, L5, and S1, via the Superior gluteal nerve6
Action
- Entire muscle: abducts the hip, stabilizes the pelvis in the coronal plane6
- Anterior fibers: flexion and internal rotation6
- Posterior fibers: extension and external rotation6
The Glute med is the “main hip abductor” due to its efficiency and strength. The Glute med is efficient since it is almost perpendicular to its lever arm8.
The glute med and glute min are both oriented mostly in the frontal plane, but the glute med is a greater abductor since it can produce ~16kg of force, which is more than 3x that of the gluteus minimus8.
The glute med’s insertional angle on the greater trochanter varies with degree of hip abduction8. At neutral, the angle is not perpendicular, thus the force generate by the glute med results in a hip abduction moment and joint compression which increases articular contact8.
As the hip moves into abduction, the insertional angle becomes more perpendicular, resulting in a greater hip abduction moment and decreased hip joint approximation force8. This trend continues until the hip reaches 35° abduction, which is exactly perpendicular8.
Overview
According to Dutton7, the gluteus medius has been nicknamed “the deltoid of the hip” due to structural and functional parallels between the two muscles.
The deltoid can be divided into anterior deltoid, lateral deltoid, and posterior deltoid7. The gluteus medius can be divided into anterior portion, middle portion, and posterior portion7.
Functionally, the anterior deltoid flexes the shoulder and the anterior portion of GluteMed flexes and IRs the hip7. The Lateral deltoid abducts the shoulder and the middle portion of GluteMed abduct the hip7. The posterior deltoid extends the shoulder and the posterior portion of GluteMed extends and ERs the hip7.
Palpation
- Position the patient in sidelying9
- Much of the glute medius and minimus overlap, but you can isolate the gluteus medius by palpating the most superior part of the iliac crest9.
- The glute med’s proximal origin extends from the PSIS almost to the ASIS9.
- The fibers of the glute med and min are fanned across the iliac crest then converge distally at the greater trochanter of the femur9.
- To palpate the gluteus minimus, dive deep to the the gluteus medius
- Having the patient actively abduct the top leg will help confirm that you are palpating the correct muscle9.
Tests & Measures
- External Derotation Test (gluteus medius tendinopathy)
Exercise
A wedge forcing the foot into hyper-dorsiflexion will cause the client to prevent excessive anterior knee translation and force more hip hinge, which will activate the glutes.
- Single leg bridge (with 90° knee flexion and pushing through the hindfoot)
- Wall triple extension
- Bridge (toes up)
- S/L Hip abduction to high knee