APTA’s Current Concepts: The Hip
Pathologies
- Fractures
- Avascular Necrosis
- Systemic Inflammation
- Infection
- Femoral Neck Stress Fracture
- Ankylosing Spondylitis
- Lumbar disc herniation
- Lumbar Radiculopathy
- SIJ Dysfunction
- Pelvic floor dysfunction
- Hip Osteoarthritis
- Hip Microinstability
- Femoroacetabular Impingement Syndrome
- Hip Dysplasia
- Greater Trochanteric Pain Syndrome
- Piriformis Syndrome
- Iliopsoas Complex Injuries
- Adductor muscle strain
- Hamstring muscle strain
Red flags
- Fractures
- Avascular Necrosis
- Systemic Inflammation
- Infection
- Femoral Neck Stress Fracture
- Ankylosing Spondylitis
- Lumbar disc herniation
- Lumbar Radiculopathy
- SIJ Dysfunction
- Pelvic floor dysfunction
- Hip Osteoarthritis
- Hip Microinstability
- Femoroacetabular Impingement Syndrome
- Hip Dysplasia
- Greater Trochanteric Pain Syndrome
- Piriformis Syndrome
- Iliopsoas Complex Injuries
- Adductor muscle strain
- Hamstring muscle strain
Lumbopelvic vs Hip
Lumbopelvic
- Ankylosing Spondylitis
- Lumbar disc herniation
- Lumbar Radiculopathy
- SIJ Dysfunction
- Pelvic floor dysfunction
Hip
- Hip Osteoarthritis
- Hip Microinstability
- Femoroacetabular Impingement Syndrome
- Hip Dysplasia
- Greater Trochanteric Pain Syndrome
- Piriformis Syndrome
- Iliopsoas Complex Injuries
- Adductor muscle strain
- Hamstring muscle strain
Intraarticular vs Extraarticular
Intra-articular
- Hip Osteoarthritis
- Hip Microinstability
- Femoroacetabular Impingement Syndrome
- Hip Dysplasia
Extra-articular
- Greater Trochanteric Pain Syndrome
- Piriformis Syndrome
- Iliopsoas Complex Injuries
- Adductor muscle strain
- Hamstring muscle strain
Red Flag Screening
Red flags as pathologies where the patient needs direct medical attention from a physician
At the beginning of your evaluation, screening out red flags is the top priority.
Hip Infection
- Hip pain
- Acute onset
- Localized redness
- Localized swelling
- Fever
Immediate attention by a physician is required
Postpone current and future PT visits
Avascular Necrosis (AVN)
- Onset: >6 weeks
- ~30-50 years old
- Traumatic MOI
- Atraumatic MOI: Hx corticosteroid use
- Decreased ROM
- Pain with weightbearing
Presents like OA but with a short onset
Warrants medical referral
Stress Fractures
Overuse injuries resulting in bony degeneration
Presentation
- Population 1: Athlete undergoing high repetitive loads
- Population 2: Osteoporosis with weakened bone structure
- Gradual onset of anterior hip pain
- Worse with activity, fully relieved with rest
- Single Leg Balance
- Single Leg Squat
- Single Leg Hopping
Stress Fx Diagnosis
Palpation is unreliable diagnostic tool due to the overlying soft tissue.
MRI is considered the gold standard for diagnosis of stress fractures.
Do not rely on XRAY results alone to rule out stress fractures.
Patellar Pubic Percussion Test
- Patient positioned in supine
- Stethoscope placed over pubic tubercle
- Tap ipsilateral patella
(+) Lack of sound propagation indicate femoral neck or pubic rami fracture
Red Flag Summary
- Lack of radiology
- Acute onset
- Trauma or a missing MOI
- Fever
- Erythema (redness)
- Edema (swelling)
- (+) Patellar Pubic Percussion Test
Ruling out other regions
- Lumbar
- SIJ
- Pelvic Floor
- Referred pain
Lumbar pathologies
Lumbar radiculopathies that result in radiating pain through and around the hip
Lumbar AROM
Consistent symptom improvement or aggravation with lumbar ROM both point towards lumbar pathologies
Using global trunk movements may not effectively isolate the lumbar spine from the hip region
Neural Tension Tests
| Test | Nerve | Roots |
|---|---|---|
| Active slump test | Sciatic | L4-5 |
| Prone Knee Flexion | Femoral | L2-4 |
Special Tests
- Active Slump Test
- Straight Leg Raise Test
- Prone Lumbar Instability Test
Limping
Patients who display a limp are 7x more likely to have a hip or hip and spine disorder compared to an isolated spine issue.
Lumbar spine DDX
- Aggravated by lumbar AROM (not global AROM)
- Dermatomal pain pattern
- Radiating pain starting proximal to the hip
- Prone Lumbar Instability Test
- Active Slump Test
- Straight Leg Raise Test
SIJ
- Fortin’s Point: Pain around the PSIS
- SIJ Compression Test
- SIJ Distraction Test
- Innominate rotation
- SIJ Thigh Thrust Test
- Sacral Thrust Test
Pelvic Floor Dysfunction
- Bowel and Bladder Changes
- Hx of Pregnancy or Birth
- Pain with sexual activity
- Pain in Pelvic region
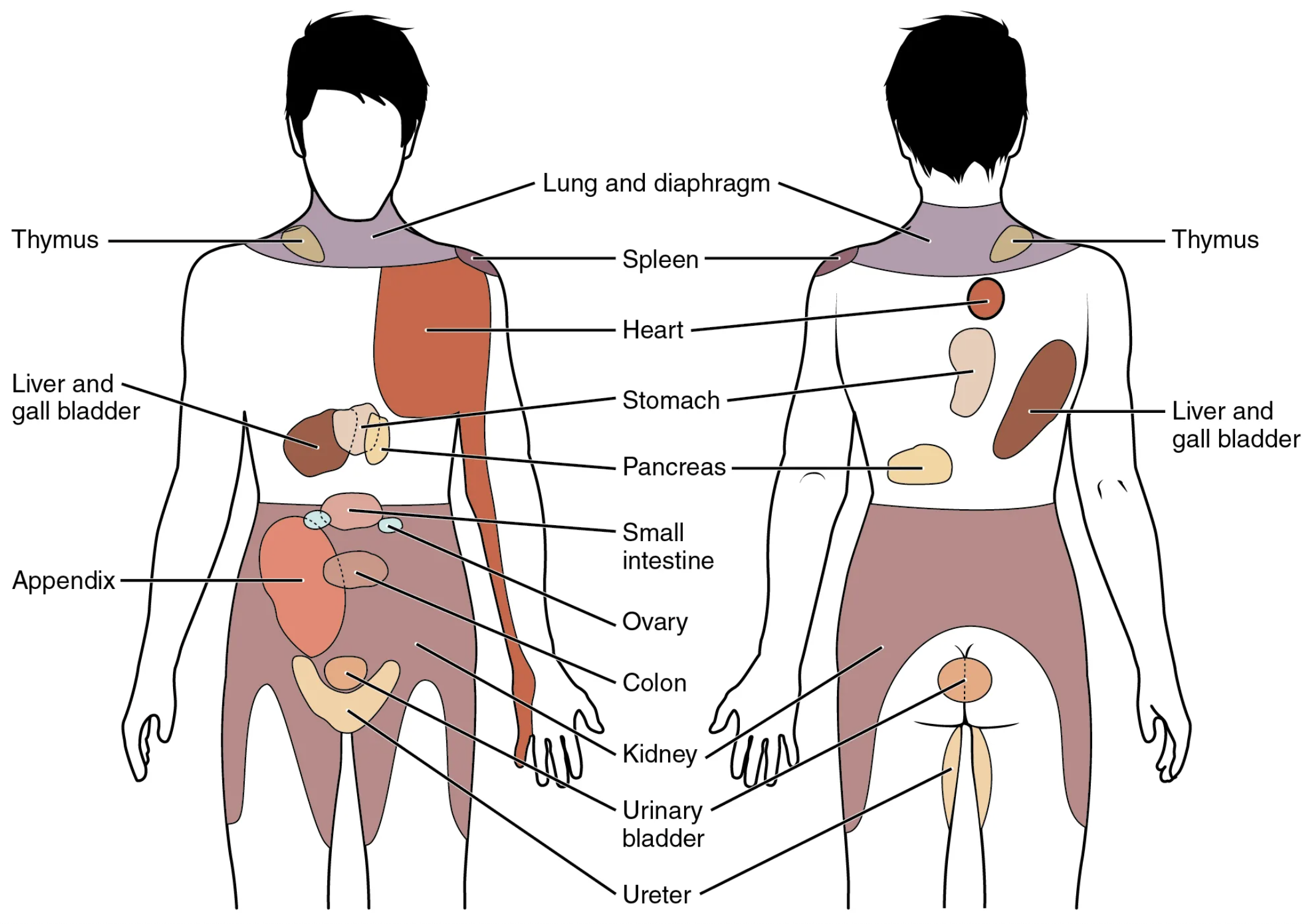
Referred pain
- Kidney
- Ureter
- Urinary Bladder
Evaluation
Range of Motion Testing
- Absolute ROM
- Comparative ROM
- Quality of end-feel
| Movement | Range |
|---|---|
| Flexion | 120° |
| Extension | 20° |
| Abduction | 40° |
| Adduction | 25° |
| Internal Rotation | 35° |
| External Rotation | 45° |
Muscle Length tests
| Test | Muscles tested |
|---|---|
| Thomas Test | Iliopsoas |
| Thomas Test (90° knee flexion) | Rectus femoris |
| Thomas Test (hip IR) | Sartorius |
| Thomas Test (Hip ER Bias) | TFL |
| Hip Adductor length test (neutral) | Adductors |
| Hip Adductor length test (90° hip flexion) | Adductors |
| Straight Leg Raise | Hamstrings |
| Ober’s Test | TFL/ITB |
Intra-articular vs Extra-articular
Intra-articular
- Hip Osteoarthritis
- Hip Microinstability
- Femoroacetabular Impingement Syndrome
- Hip Dysplasia
Extra-articular
- Greater Trochanteric Pain Syndrome
- Piriformis Syndrome
- Iliopsoas Complex Injuries
- Adductor muscle strain
- Hamstring muscle strain
- Ischiofemoral Impingement
Intra-articular vs Extra-articular
Intra-articular
- FABER Test
- Scour Quadrant Test
Extra-articular
- Adductor Squeeze Test
- Glute Derotation Test
- SLS Provocation Test
- Active Piriformis Test
- Seated Piriformis Test
Special Tests
Flexion Abduction ER Test (FABER)
- Patient in supine
- Passively bring the patient into the Figure4 position (90° flexion, 90° abduction, 90° ER)
- Note distance from knee to table
Provocation of hip pain rules in Hip joint or SIJ dysfunction
Scour Quadrant Test
Identifies mechanial hip dysfunction to rule in intra-articular pathologies such as FAIS, acetabular labral tear, and hip OA
- Patient positioned in supine
- Passively flex the ipsilateral hip to 90° flexion
- Apply an axial load along the femoral shaft
- Move the hip into more flexion and adduction
- Arc the hip into flexion + abduction
Provocation of anterior hip or groin pain rules in intra-articular conditions. Crepitus indicates abnormal intra-articular structures.
Flexion-Adduction-Internal Rotation Test (FADIR)
- Patient supine
- Passively flex hip to 90°
- Passively move to end range adduction and internal rotation
Provocation of Anterior hip pain or groin pain is indicative of FAI or Acetabular Labral injury
Log-Roll Test
Assess anterior capsuloligamentous laxity of the hip joint
- Patient in supine
- Passively ER both femurs
- Note the end position of both feet
Increased external rotation of the femur on the involved limb indicates laxity of anterior capsuloligamentous structures
AB-HEER Test
- Patient contralateral sidelying (test hip upward)
- Passively abduct the hip to 30-45°
- Hip is extended and externally rotated while the femoral head is anteriorly translated
Provocation of anterior hip or groin pain indicates anterior microinstability
Prone Hip Instability Test
- Patient Prone
- Passive external rotation and abduction
- Anterior translation of femoral head
Provocation of anterior hip or groin pain indicates anterior microinstability
Hyper Extension-External Rotation (HEER)
- Patient supine
- Contralateral knee-to-chest
- Ipsilateral knee placed in extended and externally rotated position
Provocation of at point of palpation or Radiating pain is positive for Piriformis/ deep hip stabilizer muscle dysfunction and potential sciatic nerve entrapment
Adductor Isometric Squeeze Provocation Test
- 0°, 30°, 45°, or 90° Hip flexion
- The examiner places arm between patient’s knees (if hip is flexed) or distal lower leg
- Maximal isometric contraction for 5-10 seconds
Provocation of groin pain indicates adductor muscle involvement on symptomatic side.
Provocation with hip in neutral (0°) is a contraindication for return-to-play
Gluteal De-Rotation Test
- Supine
- Passively flex to 90° and end-range ER
- Patient actively de-rotates (Returns hip to neutral rotation)
Provocation of Lateral Hip pain is a indicates GTPS secondary to gluteal tendinopathy
Active Sidelying Piriformis Test
- Patient positioned in contralateral sidelying (test hip upward) with bent knees and slight hip flexion
- Clinician palpates the piriformis muscle
- Patient performs isometric hip abduction + ER against examiner resistance
Provocation of at point of palpation or Radiating pain is positive for Piriformis/ deep hip stabilizer muscle dysfunction and potential sciatic nerve entrapment
Seated Piriformis Stretch Provocation Test
- Patient seated
- Ipsilateral heel supported and knee placed in full extension
- Passively adduct and internally rotate the flexed hip while palpating lateral to the ischium and proximally at the sciatic notch
Provocation of at point of palpation or Radiating pain is positive for Piriformis/ deep hip stabilizer muscle dysfunction and potential sciatic nerve entrapment
Hip Osteoarthritis
Hip Osteoarthritis: Progressive degeneration of the femoroacetabular joint
OA Etiology
Excessive loads on the hip
- Sports
- Heavy labor
- High BMI
Risk factors
- FAI
- Dysplasia
- PMHx joint injuries
The more risk factors a patient has, the less impact the joint will need to rule in OA
OA Presentation
- Pain in Groin and Lateral hip
- Gradual Onset
- Progressively worsening pattern
- >50years old
- ↓ Joint ROM (specifically IR)
- AM Stiffness: <1 hour after immobile periods
- Strength: ↓ LE strength
OA Special Tests
- (+) FABER
- (+) Scour Quadrant Test
- Relief with Long-axis distraction
Old OA Cluster
- Moderate anterior or lateral hip pain with weight bearing activities
- Morning stiffness >1 hour
- Hip ROM deficits:
- Hip internal rotation ROM <15°
- Hip internal rotation and flexion <15° compared to contralateral hip
- Increased pain with passive hip IR
Updated OA Cluster
- Moderate anterior or lateral hip pain with weight bearing activities
- Morning stiffness >1 hour
- Hip ROM deficits:
- Hip internal rotation ROM <24°
- Hip internal rotation and flexion <15° compared to contralateral hip
- Increased pain with passive hip IR
OA Treatment approach
Minimize joint irritation and inflammation
. . .
Short term
- Modalities
- Distraction
- Activity modification
- Gentle OKC strengthening
Long term
- Closed Kinetic Chain
- Improve hip stabilization
- Improve hip load absorption
Treatment Dosage
| Type | Days | Sets | Reps |
| Resistance | 2-3 | 3-4 | 8-12x |
| Stretching | 2-3 | 2-4 | 10-30s |
| Aerobic | 3-5 | 20-90min | 55-90% HRmax |
Refer to Aquatic Therapy
- Decreases impact of high BMI
- Minimizes joint loads
- Introduction to swimming as exercise
Femoral Acetabular Impingement Syndrome (FAIS)
Femoral Acetabular Impingement Syndrome (FAIS): Clinical presentation of hip pain caused by premature contact between femur and acetabulum bones.
Presentation
- Pain in C-Sign distribution
- Impingement positions: Repetitive/prolonged hip flexion + adduction + IR
- (+) FADIR
- Younger population
- Functional impairments
FAIS: Single Leg Squat
- Decreased depth
- Loss of contralateral pelvic height
- Genu valgum/varus
- Trunk compensations
- Poor lower extremity control
FAIS: Star Excursion Balance Test
Limited in Posterolateral and Posteromedial directions
I often use this test since it can be used as a treatment and easily added to the HEP
Treatment
There is limited literature for FAIS treatment
Sharing clinical expertise is even more valuable when managing this population!
Hip Flexor Mobility
Addressing hip flexor muscle length issues should be prioritized as tightness of these structures can have a postural effect by increasing anterior pelvic tilt.
Functional training
Progressing patients towards single-leg closed chain positions and movements
Hip Microinstability
Hip Microinstability: The combined entity of capsuloligamentous laxity and clinical symptoms (i.e. pain) with or without apprehension.
Etiology
In general there is no single traumatic event that causes hip microinstability. Bony dysplasia may be present but is not considered a necessary criterion.
The mechanism is repetitive microtrauma generally due to insufficient passive stabilization from the anterior joint capsule and iliofemoral ligament
Presentation
No hx of trauma
Aggravation with Weight bearing ER + extension (anterior instability)
Pain:
- Groin or Deep joint pain
- C-Sign Hip Pain Distribution
Functional difficulties
- Particularly in hip extension + ER
Weak hip abductor and rotator muscles
Diagnosis
- 3 Test cluster:
- AB-HEER test
- Prone instability test
- Hyperextension-external rotation (HEER) test
- 3 positive tests was associated with a 95% chance of microinstability.
DDX
Differentiate between local anterior microinstability and Global laxity
Anterior microinstability (local)
- Log Roll Test
- AB-HEER Test
- Prone Hip Instability test
- HEER Test
Global Laxity
- Beighton Scale
Beighton Scale
| Criteria | Left | Right |
|---|---|---|
| 5th finger metacarpophalangeal joint extension >90° | 0 or 1 | 0 or 1 |
| Ability to place thumb to forearm | 0 or 1 | 0 or 1 |
| >10° knee hyperextension | 0 or 1 | 0 or 1 |
| >10° elbow hyperextension | 0 or 1 | 0 or 1 |
| Ability to touch palms to floor with knees straight | 0 or 1 |
Total: /9
≥4pts → Presence of joint laxity
Adductor Muscle Injuries
Adductor muscle strains are a common injury in sports like hockey and soccer
with the MOI including acute, overuse, and acute-on-chronic
. . .
Acute Population
In kicking athletes, such as soccer, the injury is generally acute and occurs when rapidly transitioning between hip extension → flexion.
. . .
Overuse Population
Ice hockey consists of repetitive eccentric loading of the adductors and injuries are generally due to overuse
These injuries generally occur due to hip muscle weakness and lack of off-season conditioning. When ruling in an adductor strain, look for recent increases in activity
Most common adductors injured
- Adductor Longus
- Adductor Magnus
- Gracilis
Risk Factors
- Previous groin injury (2x risk)
- Lack of off-season sport-specific training
- Hip muscle weakness
- Adductor to abductor muscle strength ratio <80%
- Lower abdominal muscle weakness
- Decreased hip joint ROM
Prevention
Adductor:Abductor Strength ratio: >80%3
Pro hockey had 17x increase risk of adductor mm injury if <80%
The Copenhagen 5-second adductor squeeze test3
| Pain | Sport Readiness |
|---|---|
| 0–2 | Ready |
| 3–5 | Caution |
| 6–10 | Not Ready |
Framework for Muscle Injury Rehab
- ROM: Limited → Full ROM
- Strengthening: Isometric → Concentric → Eccentric
- Improve stabilization at nearby regions
- Maintain strength in unaffected hip musculature
Hamstring Injuries
Presentation
- Common injury in athletes
- Myotendinous junction of Biceps Femoris Long Head
- Pain and tightness in posterior thigh
Rule out Tendon avulsion
- Proximal posterior thigh pain
- Traumatic onset
- Inability or unwillingness to bear weight
- Visible ecchymosis
- Palpable defects in the hamstring musculature
H-Test
- Supine
- Perform 3x SLR’s at max ROM as fast as possible
- Rate apprehension 0-100 (most apprehension)
Delaying RTS until apprehension was at a minimum significantly reduced reinjury rates
Greater Trochanteric Pain Syndrome (GTPS)
Definition
Greater Trochanteric Pain Syndrome: lateral hip pain that may originate from numerous sources surrounding the greater trochanter3.
- Gluteus minimus and medius tendons3
- Trochanteric bursa3
- Proximal ITB3
PathoMechanism
GTPS is theorized to be an overuse injury due to chronic movement dysfunction of Hip Adduction and IR due to poor eccentric control3.
An attempt to create stability by sitting into passive structures such as IT band and glute tendons
Population
Non athlete
- 40-60 years old
- Female
Athletic
- High impact
- Jumping on hard floor
Gluteal tendinopathy
- Gluteal De-Rotation Provocation Test
- Single Leg Stance Provacative Test: Provocation of lateral hip pain is positive for GTPS secondary to gluteal tendinopathy
Piriformis Syndrome
Piriformis Syndrome: Posterior hip pain that is present with radiating pain related to piriformis activation
Four clinical signs and symptoms
- Buttock pain
- Pain with sitting
- Tenderness near greater sciatic notch
- Pain with maneuvers that cause tension of the piriformis
Special Tests
- Active piriformis test
- Seated piriformis test
My Treatment
Deep Hip Stabilizer Dysfunction
- Femoral head will be pushed forward and be passively resting on hip flexor tendons anteriorly
The long muscles will attempt to perform the job of stabilization. Long muscles such as sartorius, TFL, rectus femoris, hip flexors, and hamtrings. I think of this similar to dysfunctional deep neck flexors that result in overactive scalenes, upper trapezius, and levator scapulae.
Prone Hip IR Test
- Prone Hip IR/ER arthrokinematic test
- Symmetry
- End feel
- ROM
FAddER Contract-Relax
- Supine
- Hip flexion, adduction, & ER
- Long axis compression force
- Have the patient attempt to return the hip to neutral