Cervicogenic Headache
Cervicogenic headache is a headache characterized by referred pain to the head from cervical spine1
Epidemiology
- No genetic factor
- No familial hx
Etiology
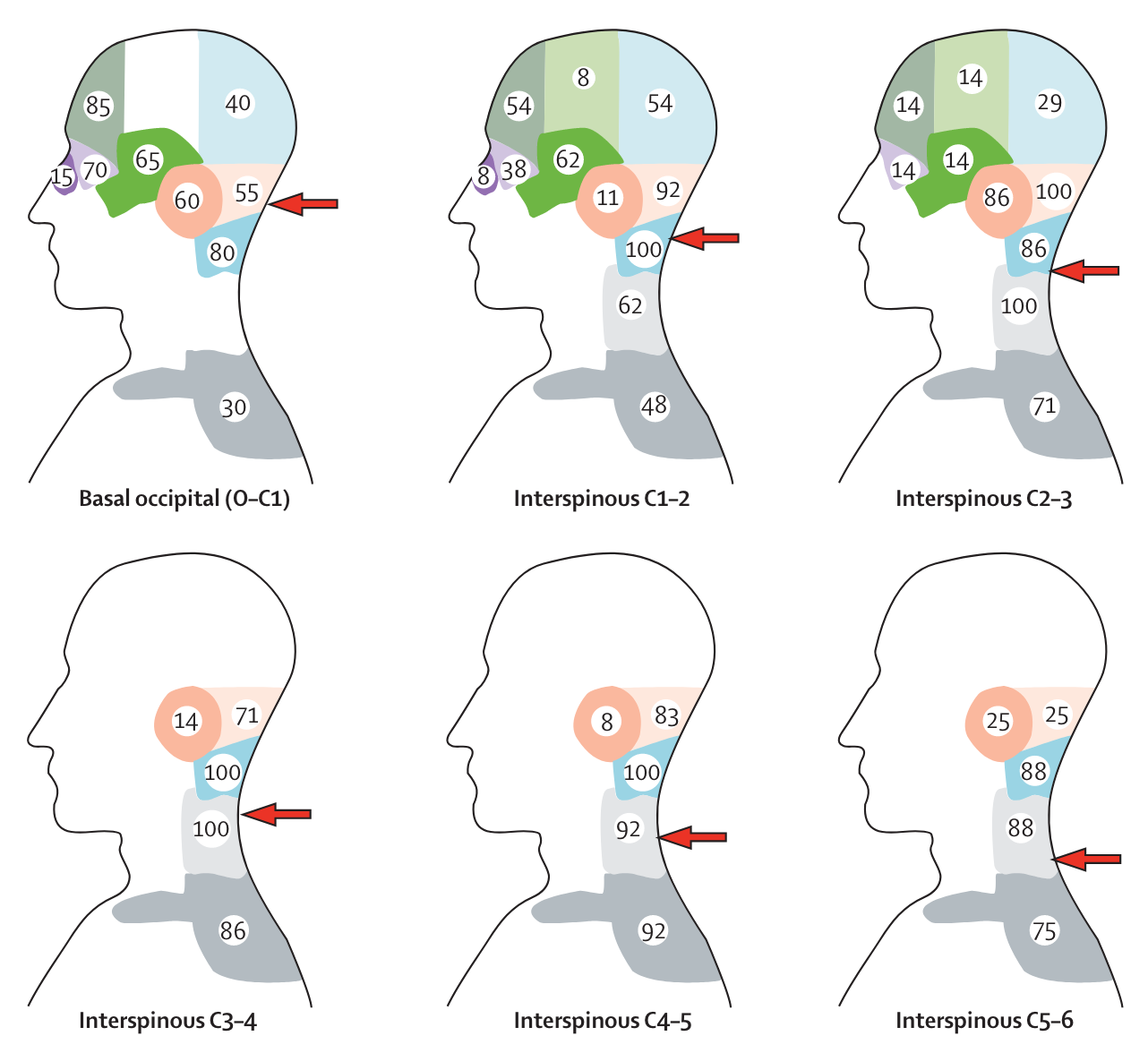
Primary cause of referred pain: Upper C/S Jt dysfxn1 - #1 (70%): C2-C3 Z-joint1 - #2 cause: C1-C21
Other mechanisms can also cause cervicogenic headaches:
- Myofascial tightness
- Stimulation of certain joints/discs in teh c spine have been shown to produce pain in the occipital region
- Pain in AA (C1-2) joint → pain is focused on occipital and suboccipital regions, and referred to vertex, orbit, and ear
- C2-C3 pain can also occur in occipital region and spread across parietal region to frontal region/orbit
Pathophysiology
A cervicogenic headache (CGH) is unilateral pain in the neck referred from bony structures or soft tissues of the neck. There is not concrete explanation for this pathology, but many authors have attempted to provide theories for the underlying mechanisms.
Bogduk’s Theory
Bogduk et al1 provided an explanation for the underlying pain:
- Convergence between cervical and trigeminal afferents in trigeminocervical nucleus1
- At the trigeminocervical nucleus, nociceptive afferents from C1, 2, 3 spinal nerves converge onto 2nd order neurons that also receive afferents from adjacent cervical nerves and from 1st division of the trigeminal nerve CNV via the trigeminal nerve spinal tract1.
Clinical Presentation
Patient with cervicogenic headaches will typicall present with lateralized, unilateral, non-throbbing headache caused by a nociceptive source in the cervical spine.
- Severity: moderate
- Irritability: high, throughout day
- Nature: dull achy of mod intensity begins in neck or occipital region that spreads to include greater part of cranium
- Stable
- Stage: insidious, chronic usually
Precipitation & Aggravation
- Neck position
- Neck movements
- Sustained positions/postures
- Especially neck flexion
- Stress
- Tension
Onset
- Occassional Warning signs
- Aura (potentially)
- May wake up w headache
- Increases as day progresses (influenced by activity)
Aggravations / Eases
- Influenced by daily activities
- Stress, tension, neck flexion, head position - can trigger or relieve
Symptoms
- Non-continuous unilateral neck pain associated w HA
Area of Symptoms
- Unilateral (may be BIL)
- Starts sub-occipital
- radiates into temporal, frontal, or retro-orbital
- Does NOT change sides
Quality
- Dulle ache or boring pain
- May have stabbing, deep pain
- Moderate to severe
Associated symptoms
- Nausea
- Vomiting
- Bradycardia
- Blurred vision
- Difficulty swallowing
- Sensitivity
- Photophobia
- Phonophobia
Subjective
Diagnostic criteria for CGH: headache with neck pain stiffness2.
- Unilateral2
- Starting from one side of the posterior head/neck2
- Migrating to the front and sometimes associated with ipsilateral arm discomfort2
Potentially bilateral head/neck pain, aggrevated by neck positions/occupations
Onset: Usually starts after neck mvmt Aggs: - Specific neck movement or sustained neck posture
- resistance/limitation of AROM/PROM or abnormal tenderness of neck mm
- pain localized to neck and occipital region that may project to the forehead, orbital region, temples, vertex or ears
- reduced strength in craniocervical extensor mm
Objective
Unilateral pain with a facet lock irradiating form the back of the head Evidence of cervical dysfunction Trigger point palpation in head/neck Aggravated by sustained neck positions Normal imaging
AROM (ext and rotation, joint dysfunction that was palpable, and cervical muscle strength in flex/ext and CCFT in pts with CGH were different compared to tension HA and asymptomatic controls (Jull et al, 2015)
The combination of palpably painful joint dysfunction at C0–C4, limited cervical spine extension, and increased sternocleidomastoid muscle activity in the CCFT yielded 100% sensitivity and 94% specificity in distinguishing CGH. (Jull et al, 2015)
Cervical flexion rotation test: Greater restriction in rotation to symptomatic side. FRT positive in all patients with C1/2 as primary symptomatic segment and negative in all other segments. (Howard et al., 2015) Firm end feel with limited ROM in upper c spine
Breathing Diaphragm dysfunction - accessory respiratory muscles lift rib cage, can be tight/hyperactive in patients with neck pain d/t deep flexor weakness.
Examination
Clinical diagnostic criteria have not proved valid but by using nerve blocks, cervical source of pain can be established1
- C/S flexion rotation test is positive
- HA reproduced w provocation of the involved upper C/s segments
- Limited C/s ROM
- Restricted upper C/s mobility
- Neck muscles impairments
- Strength
- Endurance
- Coordination
Most reliable features:
Special Tests
- Flexion Rotation Test
- “This test is used to determine the presence of a cervicogenic headache and is both a range of motion and provocation test. The patient is positioned in supine, and resting symptoms are noted. The patient is asked to maximally flex his or her neck and to hold that position. Using both hands, the clinician applies a full rotational force to both sides and notes any changes in symptoms (Fig. 25-54). The test is considered positive for a cervicogenic headache if a loss of 10 degrees or greater is noted when comparing both sides. Given the testing position, it is likely that C1–2 is the tested level. A single blind, age and gender matched, comparative measurement study by Hall and Robinson60 found this test to have a sensitivity of 86% and a specificity of 100% (QUADAS score of 12).”3
Diagnosis
Clinical Diagnostic Criteria
Bogduk (2009) Clinical criteria1
- Unilateral HA without side shift
- Symptoms/signs of neck involvement: pain triggered by neck mvmts or sustained awkward posture and/or external pressure of ipsi neck, shoulder, and arm pain, reduced ROM
- Pain episodes of varying duration or fluctuation continuous pain
- Moderate non excruciating pain, usually of non throbbing nature
- Pain starting in the neck, spreading to oculo-fronto-temporal areas
- Anesthetics blockades abolish the pain transiently provided complete anesthesia is obtained, or occurrence of sustained neck trauma shortly before onset
- Various attack related events: autonomic symptoms and signs, nausea, vomiting, ispi odema and flushing in the peri ocular area, dizziness, photophobia, phobophobia or blurred vision in the ipsilateral eye
Tests
- Manual diagnosis has not been validated1
- (+) Cervical rotation lateral flexion test
DDX
- Vascular: Dissecting aneurysms of vertebral or internal carotid arteries which can present w neck pain or headache1.
- C2 neuralgia: intermittent lancinating pain in occipital region associated w lacrimation adn ciliary injection1
Occipital Neuralgia
See4
Pharmacology
No drugs were found to be effective in treatment of cervicogenic headaches1.
Invasive Treatment
- C2-3 iv disc= cervical fusion can be effective if the pain is originating from a discogenic problem1
Steroid injections
Conservative Treatment
Overall, exercise was found to be the best treatment and all other treatments were speculative1.
Manual Therapy
- Manual therapy alone was found not to be more effective than exercise alone1
Exercise
Exercise was found to be effective1.