Pulmonary Management
Pharmacologic agents
- Adrenocortical steroids
- Antihistamines
- Bronchodilators
- Leukotriene modifiers
- Mast cell stabilizers
Note
PTs should time their treatment with the patient’s medications in mind
Surgical interventions
- Depending on pt and condition., common w cancer or lung pneumonia or fibrosis
- Wedge resection, segmental resection, lobectomy
- Pneumonectomy - whole lung removed
PT interventions
Goals
- Independence in mobility
- Maximize gas exchange (improve ventilation and airway clearance)
- Increase aerobic capacity
- Increase respiratory mm endurance
Patient education
Review the condition and offer advice on how to help patient maximize rehab or perform compensations to maximize current level of function
Bronchopulmonary Hygiene / Airway clearance techniques (ACT)
- Understand pathophysiology of condition
- ACT not always indicated
- Assess before, during and after ACT
- Vital signs before and after
- Auscultation before and after
- Combine with O2 and meds as needed
Contraindications
- Blood in lungs
- Burns
- Recent incision sites
- Lung contusion, empyema– in pleural space so NO = pleural effusion or something, dont do it! , rib fx etc can be reasons to not do airway clearance
Cough effectiveness
Medications
- Pain meds (if pain is limiting issue to the cough)
Splinting
- Use splints if they have incisions
- can be w pillow (ie heart pillow for sternal precaution)
- Provide counterpressure w arms
Positioning
- Positioning
Hydration
- Especially important with older patients
- dehydration makes secretions harder to mobilize
Examples of ACT
- Percussion
- Vibration
- Autogenic drainage
- Active cycle of breathing
- Nasotracheal Suctioning (NT)
- Flutter valves: Flutter valves should be used in adjunct to manual ACT
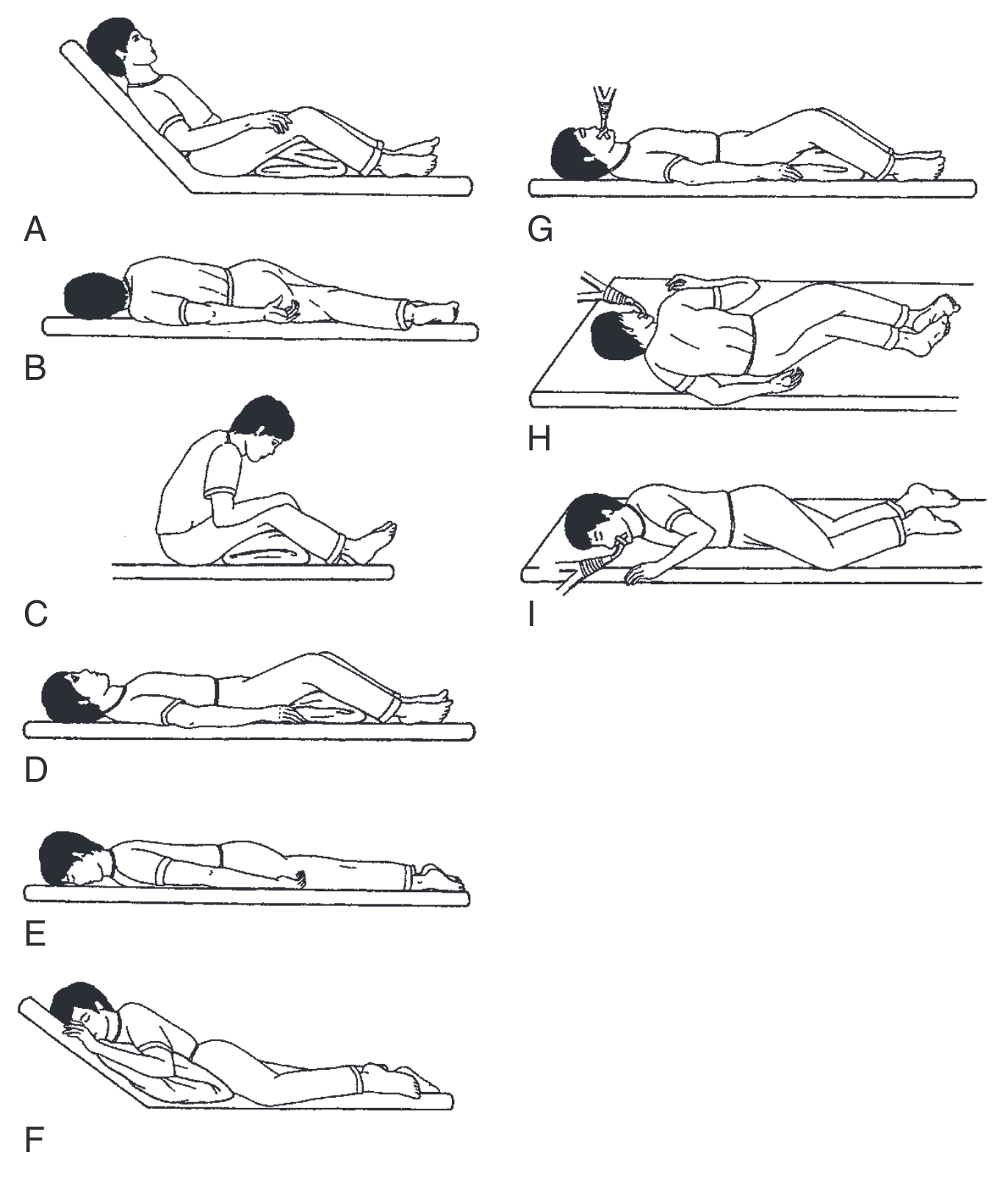
- Postural drainage (see Ch22 of Paz1)
Choosing ACT based on disorder
Obstructive disorders
- Pursed lip breathing
- Rest breaks between coughs
Restrictive disorders
- Diaphragmatic breathing
- Chest wall stretching
Activity progression
- RPE better than HR - pulmonary usually more limiting that cardiac
- Shorter more frequent sessions
- Education on energy conservation– pacing
- Document need for rests and duration of rest during txt
- Bronchopulmonary hygiene prior to exercise may be beneficial
Precautions
- Table 22.3 - test question!!!!
- Consider head position (ICP monitor – no less than 30 deg on the bed, remember certain positions can be limited)
- ICP monitoring
- Chest wall complications
- Platelets <20k (risk of bleeding w percussion)
- Osteoporosis
Percussion, Postural Drainage, and Vibration/Shaking
Benefits
Considerations
- Most beneficial when used in conjunction with additional airway clearance techniques (ACTs)1
- Patient cannot be independent with percussion or vibration/shaking; requires caregiver assistance1
- Passive1
- Time and effort intensive1
- May be uncomfortable if pain is present1
- Modification of postural drainage positions may be required with patients with increased intracranial pressure, decreased cardiac output, pulmonary hemorrhage, and severe dyspnea
- Postural drainage should be modified to remove head down positioning in infants and patients with gastroesophageal reflux disease1
Contraindications
- High intracranial pressure (>20 mmHg)1
- Uncontrolled hypertension1
- Uncontrolled or unprotected airway with risk of aspiration
- Recent esophageal surgery1
- Significantly distended abdomen1
- Pulmonary edema and/or orthopnea1
- Integumentary abnormalities over the area to be percussed or vibrated, such as burns, skin grafts, or open wounds1
- Rib fractures, flail chest, rib metastases1
- Acute hemorrhage and/or hemodynamic instability1
- Unstable head or neck injury1
References
1.
Paz JC, West MP, Panasci K, Greenwood KC, eds. Acute Care Handbook for Physical Therapists. 5th ed. Elsevier; 2020.
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Pulmonary Management.
https://yomokerst.com/The
Archive/Physiology/Pulmonary system/Pulmonary
management/pulmonary_management_overview.html