Sever’s Disease (Calcaneal Apophysitis)
Sever disease (calcaneal apophysitis) is a cause of heel pain in adolescents (8-15) with immature skeletons resulting from repetitive microtrauma due to overuse1.
Etiology
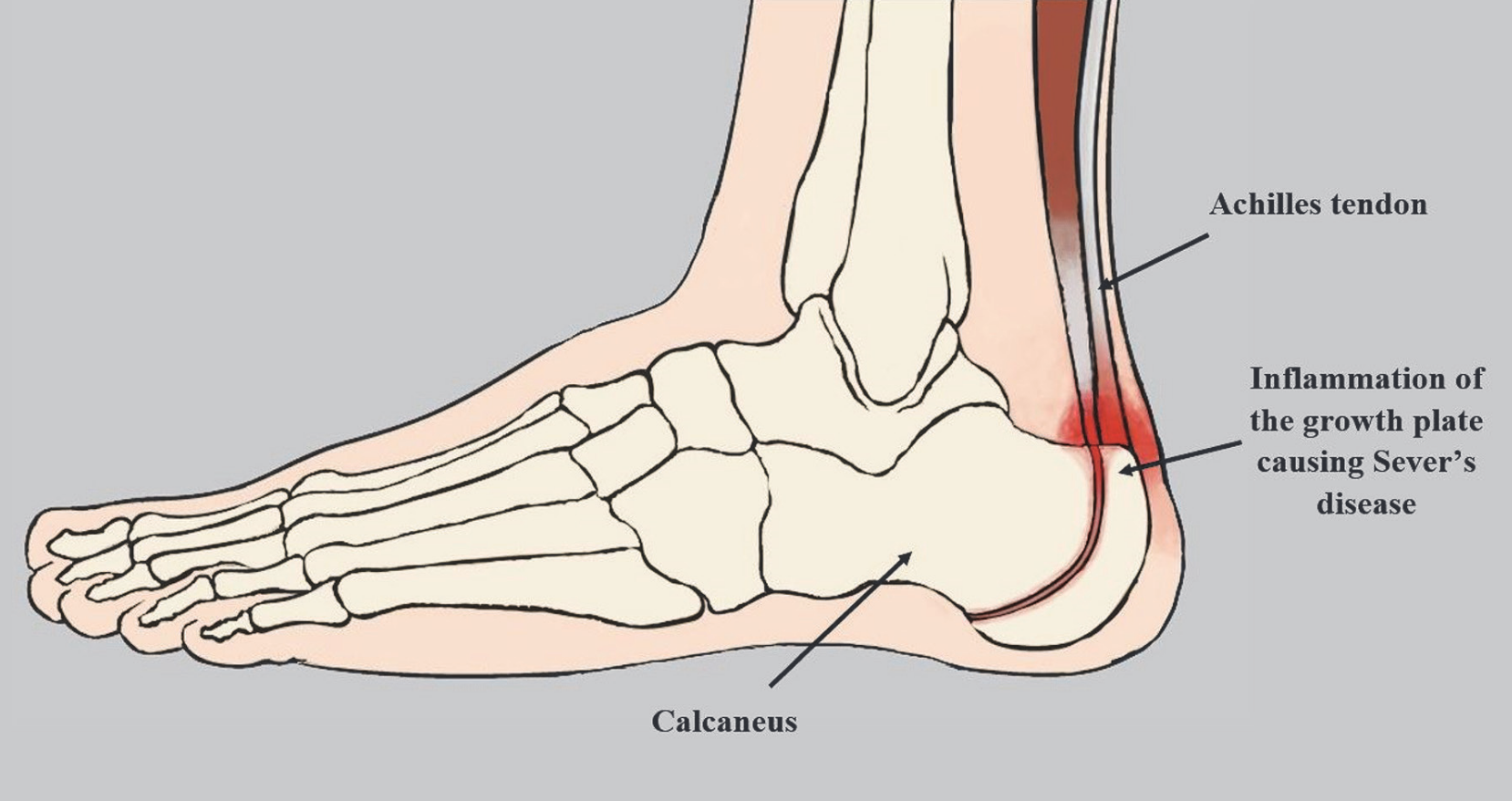
It is theorized that the early adolescent growth spurt results in significantly more bone growth comapred to the muscle-tendon unit2. As a result, this places excess stretch and tension on the the muscle-tendon unit and decreased DF ROM2. This increased tension is transmitted to the incompletely-ossified apophysis2. Over time, this stress can irritate the growth plate (physis) resulting in inflammation (calcaneal apophysitis)2.
The microtrauma of Sever’s Disease can be caused by repetitive strain and microtrauma of the strong Achilles tendon on the relatively soft calcaneal apophysis1.
Increased Achilles Tendon Tension
A shortened triceps surae directly correlates to the irritation of the apophysis1.
Factors Impacting Severity
- High BMI1
- Limited ankle range of motion3
- Activity
- Increased/excessive sports activity1
- Running on hard surfaces
- Shoewear
- Poorly cushioned or worn-out athletic shoes1
- Cleated athletic shoes
- Biomechanics
Sever disease is not generally associated with traumatic events; however, in rare cases, trauma may lead to a complete avulsion fracture.[10] ’
Epidemiology
- Sever’s Disease is one of the leading causes of heel pain in adolescents1.
- Sever disease contributes to 2% to 16% of all musculoskeletal complaints in children1
Sports
The most prevalent sports associated with this condition involve repetitive running and jumping
Age
Sever’s Disease primarily occurs during the rapid growth phase from ages 8-15 years old1.
Gender
- Males are more likely to develop this condition (2-3:1)1.
Onset
- The typical age of onset is around 12 for males and 11 for females.
Pathophysiology
Normal
The posterior calcaneus develops as a secondary ossification center that provides the attachment point for the Achilles tendon. During the early adolescent growth spurt, bone growth exceeds the ability of the muscle-tendon unit to stretch sufficiently to maintain previous flexibility.
Why the apophysis?
Consequently, increased tension is exerted across the unossified or incompletely ossified apophysis. The apophysis represents the most vulnerable point in the muscle-tendon-bone attachment, unlike the tendon in an adult. Therefore, the apophysis is susceptible to overuse injuries resulting from repetitive stress.
Traumatic Stimuli
“Repetitive and excessive traction exerted by the strong Achilles tendon leads to microtrauma and chronic irritation, resulting in thickening and pain at the apophysis”1.
Theoretical Mechanism
Current theories attribute Sever disease relies on the ongoing shear stress and repetitive impact on the open calcaneal apophysis.
Presentation
Most Sever’s disease patients will present as an active (8-15y/o) experiencing unilateral or bilateral heel pain aggravated during and after activities such as running and jumping1.
Unilateral vs Bilateral
Up to 60% of patients experience pain in both feet
MOI
Generally, there is no specific MOI1.
Onset
Observation
Palpation
- Tenderness at Achilles insertion on the heel1
PROM
- Pain with DF PROM1
Pain can be reproduced with manual medial and lateral compression of the posterior calcaneus and aggravated by standing on tiptoes—a phenomenon known as the Sever sign
DDX
Sever’s disease, retrocalcaneal bursitis, Achilles tendonitis, osteomyelitis, and plantar fasciitis2
Running Considerations
Running is a risk factor for Sever’s Disease since children who primarily run tend to experience in muscular imbalances2.
Stronger muscle groups
- Strong plantar flexors
- Knee extensor muscles
Weaker Muscle groups
- Weak knee flexors
- Dorsiflexors
These imbalances cause an increased strain on the muscle-tendon-bone attachment during physical activity, which predisposes to Sever’s disease.
Assessment
- Children with Sever’s disease have increased normalized cadence while running, which could be a subconscious attempt to decrease the peak plantar pressures and subsequent pain2.
Prognosis
Treatment
Orthotic
- Soft heel lift in order to decrease impulse and peak force