| Other presentations of functional tremors | |
|---|---|
| Item | Phenotype |
| Optional Features | |
| Ballistic suppression | Brief arrest of tremor with performance of a ballistic movement in the opposite limb |
| Dual task interference | Disruption in tremor frequency and amplitude when simultaneously executing a competing task |
| Increase amplitude with weight loading | Tremor amplitude increases with increasing weight applied to limbs |
| "Whack-a-mole" sign | Spread of tremor to another body part when restrained by the examiner’s hand |
| Other functional signs or phenotypes | Give-away weakness, non-dermatomal hypoesthesia, associated functional gait disorder, functional dystonia, etc |
| Universal features | |
| Frequency variability | Tremor frequency changes throughout examination |
| Entrainment or full suppressability | Tremor either disappears (suppressability) or adopts the frequency of a repetitive task elsewhere (entrainment) |
| Distractibility | Tremor amplitude attenuates when attention is driven away from affected body part |
| Tonic coactivation | Co-contraction of antagonistic muscles immediately prior to reemergence of tremor |
| Source:5 | |
Functional Neurologic Disorder (FND)
History of FND
Conversion Disorder
These disorders were traditionally termed “Conversion disorder” by Freud and his followers to describe the conversion of “psychic energy” into physical symptoms1
Psychogenic Neurologic Disorder
2 types of clinical psychogenic neurologic disorders:
Note
Both of these disorders are considered to have no physical explanation of symptoms1
Chronic illness + Classical Hysteria
- A chronic illness marked by multiple and often dramatically presented symptoms and somatic abnormalities of “classic hysteria,”
- Predominantly in women (there is potential sexism and acquisition bias in this categorization but we report our and our colleagues contemporary experience) and
Compensation Neurosis
- Inexplicable disability or symptomology
- Individual is obtaining compensation, influencing litigation, avoiding military duty or imprisonment, or for the manipulation of some other interpersonal or societal situation.
- This latter state has been called compensation neurosis, compensation hysteria, or hysteria with sociopathy, in other words, malingering.
- Predominantly of men but also of women who
Pathophysiology Framework of FND
Note
Through studies, it has been shown that functioning of brain is different than feigning2.
FND has been described as dysfunction across brain circuits3. Of these brain circuits, 5 constructs have been created3.
Emotion processing (salience)
Dysfunction in the emotional processing construct manifests as emotional reactivity, deficits in emotional awareness (ie physiological arousal in absence of emotional arousal), amplification of FND symptoms in some mood states (ie panic, shame), aberrant salience processing, etc3.
Agency
Dysfunction in Agency manifests as impairment in belief/circuit around: Pt is agent of action/Free will → produces voluntary movement3. Movement lacking self agency is experienced as involuntary3. These involuntary movements are clinically deemed functional tremors or functional seizures, but the brain areas generating these movements are the same ones involved in the production of voluntary movements3.
Attention
Attentional perseveration is defined as the “tendency to focus on a physiological system to the neglect of other systems, and an impaired ability to adaptively, volitionally shift attention3.” This concept is analogous to hemineglect syndrome wher patients can attend to his/her unaffected body parts but this focus is considerably difficult and requires conscious effort3. Likewise, patients wtiAllocate attentional resources to threat stimuli (ie angry faces) (especially those with functional seizures)
Interoception
Interoception refers to a process by which the nervous system senses/interprets/integrades internal body signals into conscious and unsconscious perceptions of sensation3. In FND, the percetion produced through interoception can be abnormally enhanced or diminished3. Abnormal interoception sensations can materialize as attenuated visual, auditory, or skin sensitivity3. Abnormal interoception can impact movements and result in tremors, dystonia, seizures, and weakness3.
Predictive processing/inference
Predictive processing/inference refers to the process by which a person generates beliefs about cause/effects of events within/outside body3. Environmental conditions can rapidly alter this process3. FND patients with this dysfunction can demonstrate erroneous perceptual inference (about sensorimotor or emotionally valenced phenomena), and their beliefs become reality3.
Abnormal sensory input
updated by sensory input that indicates it IS there
Subjective
History
Note
Due to the importance of MOI and risk factors, the subjective should Focus on predisposing, precipitating and perpetuating factors!2
- Adverse experience in childhood/recently? (very common)
- Attachment theory (life growing up)
- Consider: Social/cultural norms, life experiences, religion, language, stress
- Psychological comorbidities
- Comorbidities
Other medical evaluation
Mechanism of onset
Functional limb Weakness
- Functional limb weakness
- Expect: voluntary movements are hard while automatic ones are preserved. Also expect that there is a global pattern- affects flexors/extensors equally2
Involuntary movements
- Functional tremor?
- aggs/eases?
- Functional seizure:2
- any urinary incontinence/physical injury? Seizure plan?
- Any precursors like autonomic arousal? → note:
Note
functional seizures can be seen as an involuntary, learned brain “reflex” that gets rid of unpleasant sensations. Can explain to patients this way.
Note
Side note: No medications (seizure meds) should be used as it can exacerbate events → as much as 40% of pts with functional seizures can improve with meds (however, likely placebo effect)2
Functional dystonia
- Presence
- Aggravating factors
- Easing factors
Urinary retention/scan negative cauda equina
- CBT usual tx2
Functional cognitive symptoms
- Memory problems?2
Note
Memory problems in FND are likely d/t attentional deficits (lapses in concentration)2
- Metacognitive error is prominent in the form of catastrophic negative self evaluation of one’s own cognitive performance (up to 24% of pts attending memory clinics may have functional cognitive disorder)2
- Examination of behavior and language during consultation discriminates functional from degenerative cognitive symptoms – those with functional cognitive disorder are likely to attend meetings alone, be distressed, give rich/specific accounts of memory failures compared to those with neurodegenerative disease2
- CBT helpful, contextualizing memory lapses that fall within normal, tackle unhelpful avoidance, and excessive/counterproductive use of memory aids/strategies (think post its etc). Also treat comorbid anxiety/depression as common2.
Other symptoms
- Fatigue? Sleep disturbance? Concentration symptoms?2
- Speech problems (dysarthria, mutism, foreign accent syndrome), sensory problems (numbness/positive sensory symptoms, especially with motor symptoms) , hearing loss/sensitivity, visual loss/diplopia, globus, PPPD (chronic dizziness)2
APTA Recommendations
Per APTA may be beneficial to ask:
- Does the disorder produce more attention from a spouse?
- Does the disorder mean that the patient does not have to return to a job that she/he did not like?
- Is the amount of money received with disability insurance more, or more secure, than what the patient might get by working?
- Does the patient know how to get a job or what job she/he has sufficient expertise to do?
APTA’s red flags
Per APTA- Red Flags suggesting FMD
- Adult age of onset
- Paroxysmal tremor as predominant clinical feature
- High phenomenological variability between episodes
- Rapid and maximal severity
- Precipitation of attack or increase in symptom severity during examination
- Atypical and variable duration of attacks
- Presence of multiple atypical triggers
- Altered level of responsiveness
- Presence of odd precipitating factors
- Presence of unusual relieving maneuvers
- Additional functional physical signs or medically unexplained somatic symptoms
- Atypical response to medication
- Presence of somatization
Objective
Functional limb weakness
Note
Note/Pt edu: Functional leg weakness → pt does not sense that limb IS there, opposite of phantom limb syndrome. Abnormal brain prediction that leg is not there, which overrides/fails to be updated by sensory input that indicates it IS there2
Hoover’s sign
A clinician can check for Hoover’s sign in order to differentaite between general hip extension weakness and functional hip extension weakness.
Technique (assuming the L hip is demonstrating weakness):
- Patient goes into hip extension against resistance with L leg
- Test patient’s ability to perform resisted hip flexion on the right leg which indirectly tests hip extension on the left leg.
- If the patient has L hip extension weakness against direct resistance, but has sufficient strength against resistance with R hip flexion, this is considered positive
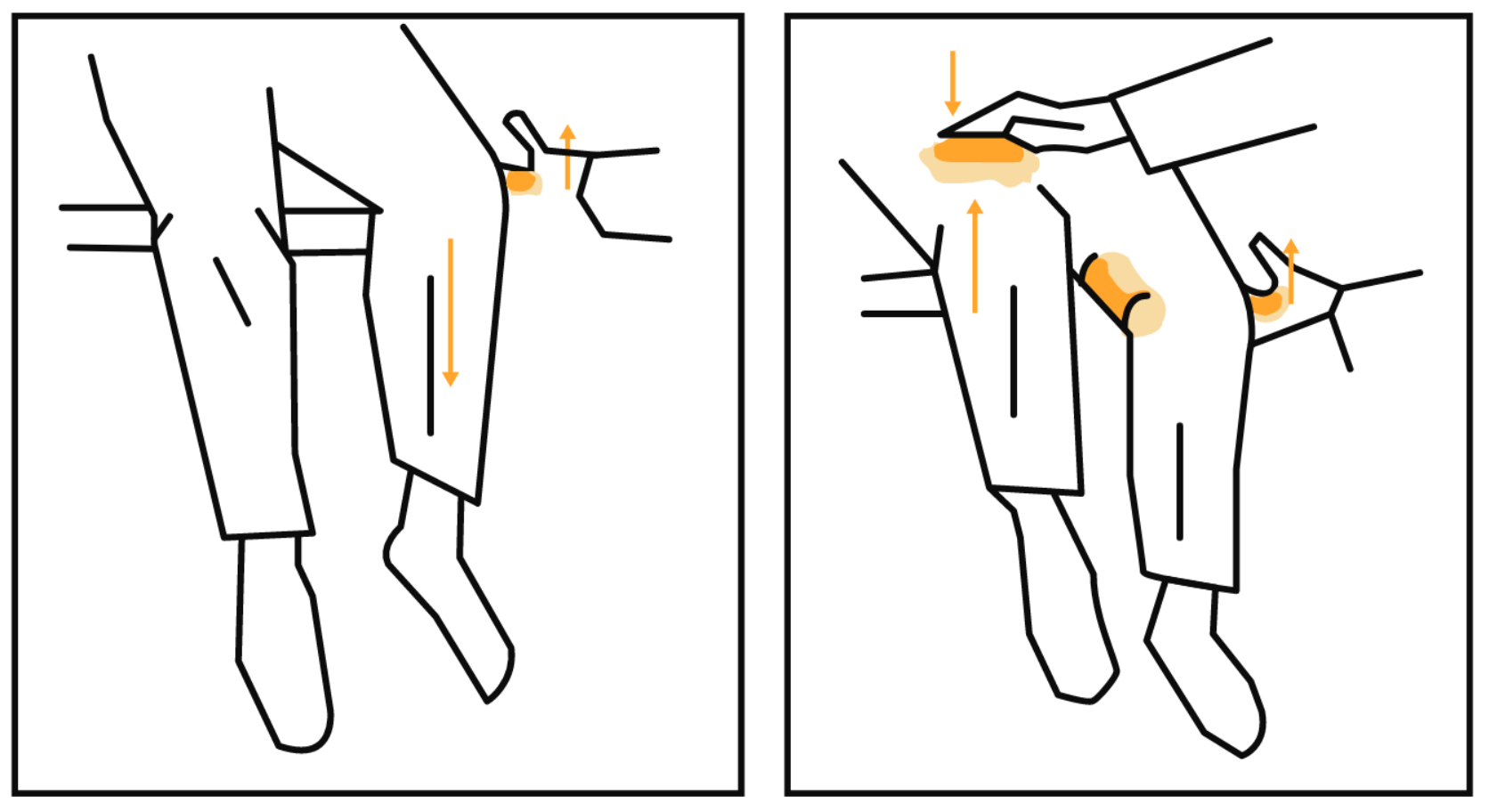
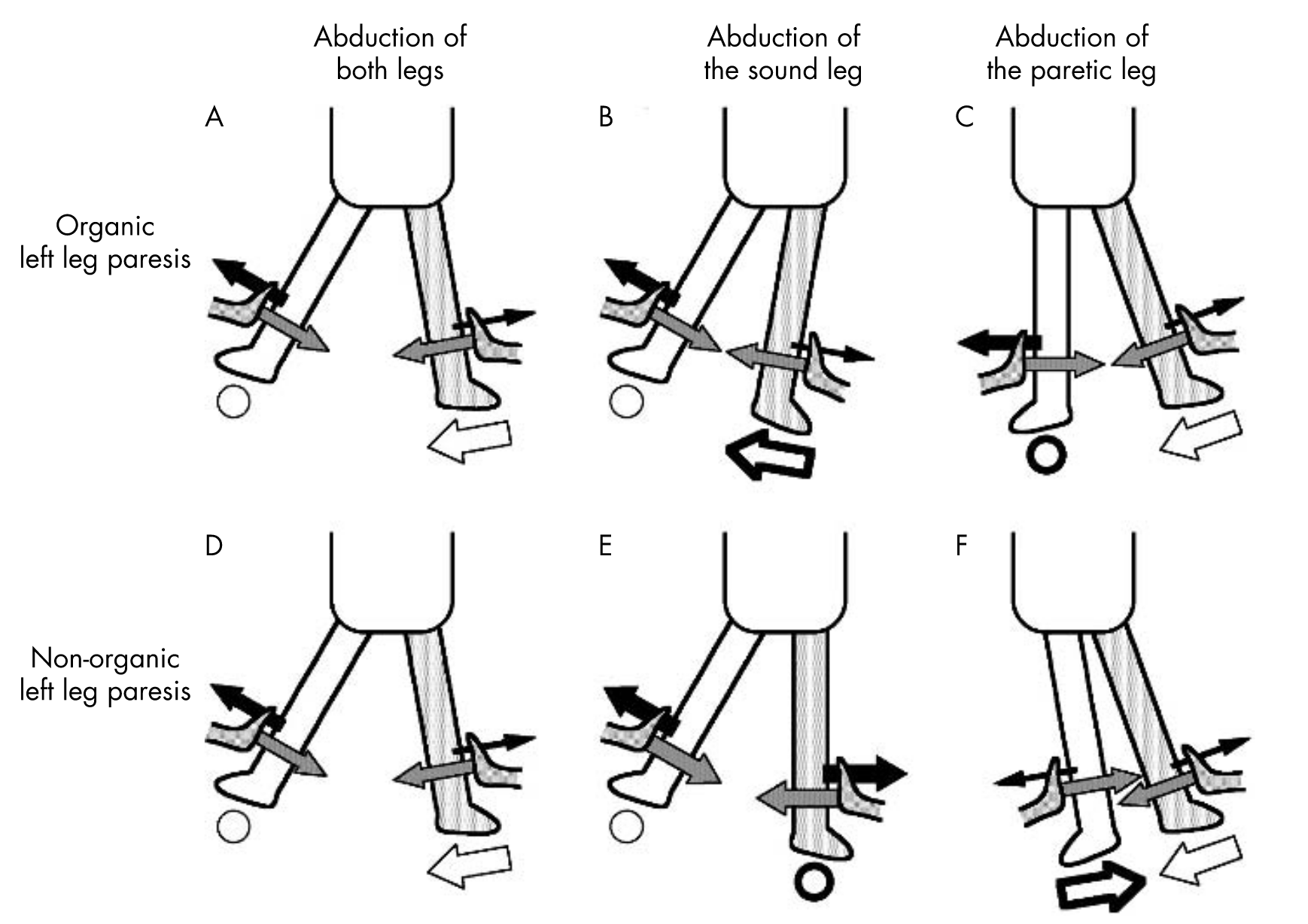
Hip Abductor Sign
Weakness of hip abduction that returns to normal with contralateral hip abduction against resistance
Arm Drop Test
Patient is positioned in the supine. Ensure the patient’s face is shielded (in case of an organic etiology). Lift the patient’s plegic arm, suspending it over the patient’s face, then suddenly dropping the arm. If the patient has FMD, the patient will deflect the arm from hitting the face in the case of FMD.
Functional limb weakness should be treated with patient education
Functional Tremor
In the arms, ask the patient to copy a rhythmical movement made between finger/thumb using their better hand2. In the legs, ask the patient to copy foot tapping2. And in the neck, have the patient follow movements of your hand with their tongue2.
In a functional tremor, one should expect to see variable frequency (not amp) tremor that changes dramatically during externally cued rhythmic movements2. If the tremor on the other hand stops, entrains to the same rhythm, or pt has difficulty copying movement → consider functional tremor2.
Note
While a functional tremor will entrain with distraction, an organic tremor will typically increase in amplitude with distraction. Entrainment can result in remission in FMD during distraction maneuvers with uninvolved limbs
Note
Many movement disorders worsen with stress/disappear with sleep → do not rely on these sx for a diagnosis
Functional Dystonia
Functional dystonia can presenta s fixed abnormal posture, but other forms are usually mobile2
Can present as:
- Inverted/PF ankle
- Flexion of fingers
- Face dystonia (jaw deviation to one side + contraction of platysma + lip curl down/upward + facial weakness + contraction of orbicularis oculi can be present + eyebrow lowered on affected side2)
Functional dystonia commonly results in secondary symptoms of pain which can severely impede with ADLs2.
Functional Seizures
Signs of functional/dissociative seizures:
- Longer duration >90 seconds2.
- Fluctuating course2.
- Asynchronous movements2.
- Side to side head or body movement2.
- Closed eyes2.
- Memory of the event2.
Signs for epileptic seizures
Functional Sensory symptoms
Yes/No Test
In the yes/no test, the patient is asked to say “yes” when they detect a stimulus and “no” when they do not detect a stimulus. A response of “no” immediately after a stimulus may indicate a nonorganic sensory loss. A response of “no” would suggest that a functional disorder is not present, as a truly anesthetic patient would not feel anything and therefore would not respond.
Forced choice test
In the Forced-Choice test, the patient is asked to distinguish between a sharp or dull stimulus, and an upward or downward movement of a toe or finger. A percentage of correct responses in a series of trials that is less than that observed by chance may indicate nonorganic sensory loss.
Interventions
Note
Note: many have negative experiences with healthcare → education is key about their brain/NS functioning. Never use a “nothing wrong” accusation. Finding a root cause is uncommon, as it is multifactorial
Patient Education
Communication of diagnosis/understanding
Example
“FND is a problem with the functioning of the NS, a problem with the software, not the hardware”2
Limb weakness
Example
After Hoover’s sign
”Did you see how your leg returned briefly to normal when I did that test (Hoover’s sign). That shows us that there is a problem with the way your brain is sending the signal to your leg (voluntary movement), but the automatic movements are still okay”2.
Limb blindness
Example
“Have you heard of phantom limb syndrome? That’s when someone has an amputation, but their brain still thinks the limb is there. FND is a bit like the opposite, the leg/vision/sensation is there but the brain thinks it isn’t anymore. The map of that part of the body in the brain has gone wrong”2.
Weakness/movements
Example
“Functional brain scans have shown that the brain is working too hard in FND. Normally we shouldn’t have to think about how to move our arms our legs. As soon as our brains start to work on this too hard it goes wrong. It’s similar to thinking about your feet when you are climbing upstairs, or trying too hard to fall asleep at night”2.
Seizures
Example
“Functional seizures are when the brain goes into a trance-like state called “dissociation” suddenly, all by itself. This is the medical word for being cut off or distant from your surroundings. That’s a bit like the feeling you have just before your seizures sometimes. We think it does this as a “reflex” response – sometimes to get rid of a horrible feeling that many people report just before. After a while, it will often happen for no reason and when people are most relaxed”2.
Dystonia
Example
“Your brain thinks that the foot is straight even though it’s turned inwards. That’s why it’s hard for you to keep it in a straight position”2.
Note
Cervical dystonia clinical pearl from ReActive PT instagram page:
- Skipping with scarves
- Scarves are a great external focus for eyes/head movement (great for automatic head movements)
- Postural responses : bouncing, skipping, dancing, moving on a tilt board/bosu can all help with automatic responses
- Postural righting responses = automatic head movement
Associated pain
Example
“Chronic pain is usually due to an ‘increased volume knob’ in the pain pathways throughout the nervous system, but especially the brain. This is called ‘central sensitisation’ and, like FND, is also a problem with abnormal nervous system functioning”2.
Prognosis
Note
“It is not an easy problem to put right, many factors affect it, but there is a potential to improve and many do make a full recovery”2.
How physical therapy can help
Example
“Physiotherapy can help ‘retrain’ the brain in FND. It works best when we can use those principles of distraction that I showed you. A physiotherapist may ask you to try to speed up the movement or do it in an unusual way, to music or in a mirror. Somewhere in your brain we think the automatic movements are in there, and we need to coax them out”2.
Psychologists
Note
“It is common in FND for people to have problems like anxiety and depression. This can be a consequence of having the symptoms but, in many, it is already there for other reasons. FND symptoms make people fearful of falling and being injured and of being embarrassed. For some, there are things that have happened which may explain why your brain is vulnerable to going wrong in this way and could be worth exploring. I think a psychiatric/psychological assessment could be helpful. What do you think?”2
Patient Resources
Functional MOTOR disorder (FMD) (what PT treats!)
Note
based on6
Consensus recommendations
General Treatment Principles
- Build trust before challenging the patient6.
- Limit hands on treatment, facilitate- do not support6.
- Encourage early WB (bed strength does not correlate with ability to walk/stand)6.
- Foster independence/self management with goals6.
- Goal directed rehab - focus on functional/automatic movements (ie walking) rather than impairments (weakness) and controlled (requiring lots of attention) movement (like strength/non automatic movements)6.
- Minimize use of maladaptive patterns/positions (retrain with correct biomechanics)6.
- Avoid adaptive equipment/aids unless absolutely necessary (never recommend splints)6.
- Challenge / recognize unhelpful thought patterns6.
- Develop a relapse prevention plan6.
- NEVER say psychogenic/conversion disorder, use functional movement disorder or weakness/paralysis/tremor/dystonia etc6.
- Acknowledge that their symptoms are real, and not imagined6.
- Acknowledge that these symptoms are common and you FREQUENTLY see patients with these symptoms (trust is huge, they need to buy in completely)6.
- Explain that their symptoms can get better : the problem is with NS functioning and not actual physical damage to the NS6.
- Explain that FMD is diagnosed with clinical signs which demonstrate normal movement is possible, and physical therapy can help coax out the automatic movements that were once within your brain. (through distraction, music, etc)6.
- Clinical signs: hoovers, hip abductor sign, abolishing tremor with rhythmical movements6.
- Explain a wide variety of factors can cause symptoms → physical illness, injury, psych factors like anxiety/depression/trauma6.
- PT can retrain the NS to regain control over movement6.
Language
- Correctly remove blame/fault/voluntariness6.
- “Brain is attending to your body in an abnormal way, your tests show that your muscles are capable of movement, but we have to retrain your nervous system to allow that movement to happen”6.
- To cue “ALLOW your leg to come forward”, do not say: “step your leg forward”6.
Treatment ideas
- Retrain movement through diverted attention6.
- Minimize self focused attention by distracting/preventing the patient from cognitively controlling movement and to stimulate automatically generated movement6.
- Can be achieved by altering focus of motor attention, such as thinking about a different part of the movement or trying FAST, RHYTHMICAL, UNFAMILIAR, OR UNPREDICTABLE MOVEMENT6.
- Distraction
- OTHER ideas to normalize movement:6.
Treatment Plan
Mechanism
Symptoms
Note
functional seizures can be seen as an involuntary, learned brain “reflex” that gets rid of unpleasant sensations. Can explain to patients this way.
References
1.
Ropper AH, Samuels MA, Klein J, Prasad S. Adams and Victor’s Principles of Neurology. 12th ed. McGraw Hill; 2023.
2.
Bennett K, Diamond C, Hoeritzauer I, et al. A practical review of functional neurological disorder (FND) for the general physician. Clinical Medicine (London, England). 2021;21(1):28-36. doi:10.7861/clinmed.2020-0987
3.
Drane DL, Fani N, Hallett M, Khalsa SS, Perez DL, Roberts NA. A framework for understanding the pathophysiology of functional neurological disorder. CNS spectrums. Published online September 2020:1-7. doi:10.1017/S1092852920001789
4.
Sonoo M. Abductor sign: A reliable new sign to detect unilateral non-organic paresis of the lower limb. Journal of Neurology, Neurosurgery, and Psychiatry. 2004;75(1):121-125.
5.
Schwingenschuh P, Espay AJ. Functional tremor. Journal of the Neurological Sciences. 2022;435:120208. doi:10.1016/j.jns.2022.120208
6.
Nielsen G, Stone J, Matthews A, et al. Physiotherapy for functional motor disorders: A consensus recommendation. Journal of Neurology, Neurosurgery, and Psychiatry. 2015;86(10):1113-1119. doi:10.1136/jnnp-2014-309255
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Functional Neurologic
Disorder (FND). https://yomokerst.com/The
Archive/Neuroscience/Neuropathology/Functional Neurologic
Disorder/functional_neurologic_disorder_FND.html