Hand MSK
Musculoskeletal overview
Carpal bones
- Proximal carpal row:
- Distal carpal row:
- Pisiform
Scaphoid bone
The scaphoid bone Articular surfaces:
- 2 distal convex surfaces to articulate with:
- 1 concave articular facet: to articulate with the capitate
Stabilization
- 1st factor
- scapho-trapezial ligament
- Scapho-trapezoidal ligament
- Scapho-capitate ligament
- 2nd factor
- Radio-capitate ligament extends from anterior border of the radial styloid process to the anterior aspect of the capitate2.
- 3rd factor
- Tendon of FCR runs anterior to the scaphoid as it courses distally to its distal insertion on the 2nd metacarpal2.
Scaphoid tilting
- When in flexion the scaphoid lies flat:
- The scaphoid is jammed between the distal trapezium and trapezoid and the proximal radius2.
- The inferior pole of hte scpahoidslides on the proximal articular surfaces of the trapezoid and trapezium2.
- While this occurs, the anterior ligaments tension and limit excessive anterior movement2.
- Simultaneously, the proximal scaphoid is blocked by the posterior border of the radius2.
- When the lateral pillar is stretching
- The contraction of FCR helps to limit excessive elongation of the pillar2.
Read more about the scaphoid bone here
Lunate
The lunate bone is asymmetrical due to its thickened anterior aspect and thinner posterior aspect2. This asymmetry changes the effective distance between the capitate, lunate, and radius2.
-
In neutral : the distance between these 3 bones corresponds to the average lunate thickness2 -
In extension : The distance is decreased due to the less bulky posterior aspect of the lunate2 -
In flexion : The distance increases due to the bulkier anterior aspect of the lunate
- Articulation
- Concave distal surface of lunate articulates with the convex capitate head2
Read more about the lunate bone here
Triquetrum
- Articulation
- Concave distal surface of triquetrum articulates with the concave proximal surface of hamate2
Read more about the triquetrum bone here
Trapezium
- Articulation
- Concave proximal surface articulates with the convex, distal surface of the scaphoid2.
Read more about the trapezium bone here
Trapezoid
- Articulation
- The proximal concave surface of the trapezium articulates with the convex distal surface of the scaphoid2.
Read more about the trapezoid bone here
Capitate
- Articulation
Read more about the capitate bone here
Hamate
- Articulation
Read more about the hamate bone here
Pisiform
Read more about the pisiform bone here
Midcarpal Joint
Although the midcarpal joint is made up of many bones, it is best to simplify the hand:
- Each row of carpal bones as a single structure
- Divide the midcarpal joint into a lateral and medial part
- Lateral part: forms a plane joint between the distal trapezium and trapezoid articulating with the scaphoid2
- Medial part forms a condyloid joint consisting of the capitate head and hamate forming a convex aspect that articulates with the concave surface formed by the 3 proximal carpal bones2.
Neutral position
In the midcarpal joint’s neutral position, the hand is straight.
In this position, the scaphoid and distal surface of the radius are in contact2. The scaphoid and center proximal surface of the trapezium are in contact2.
- Ligaments
Extension
As the midcarpal joint moves from neutral to extended, the distance reduces and the trapezium moves posteriorly2.
- Contact between the articular surfaces of distal radius and the scaphoid2.
- Contact between the trapezium and scaphoid2.
- Anterior ligaments increase tension2
Flexion
During flexion, the distances between the radius and trapezium also reduces when moving from neutral to flexion2.
- Moving into flexion, the scaphoid lies flat and most of its contact is on the posterior aspect of the radius2.
- During midcarpal flexion, the trapezium slides proximally and anteriorly on the distal scaphoid2.
Scaphoid-lunate couple
The wrist flexion-extension movement divides into 3 sectors:
- first 20° from neutral: The movements ar small, the ligaments are slack, and intraarticular pressure is minimal2.
- 40° from neutral: the ligaments being to stretch and intraarticular pressure rises
- Up to this point, the movements involving the wrist and midcarpal joint have roughly the same range2.
- 80° from neutral: Ligament tension and intraarticular pressure reaches a maximum2.
Beyond section 3, the ligaments tear and damage. These damages may go undetected. This can lead to instability, fracture, and dislocations2.
Locking scaphoid pillar
Locking lunate pillar
Muscles of the wrist
- Anterior wrist muscles
- Posterior wrist muscles
- Groups
- Group I
- Group II
- Group III
- Group IV
Metacarpal and phalangeal bones
There are 5 metacarpal bones, 1 for each digit.
In terms of
The metacarpals have distinct osteologic features:
-
Base : Proximal end that articulates with the carpals3 -
Shaft : Between the base and neck3 -
Neck -
Posterior tubercles : Attachment for the collateral ligaments3 -
Head : Convex articulation for proximal interphalangeal joint3
1st Metacarpal
The “1st metacarpal” is part of the thumb and is the shortest and stoutest3.
Read more about the 1st metacarpal here
2nd Metacarpal
The 2nd metacarpal is generally the longest
Read more about the 2nd metacarpal here
Read more about the 3rd metacarpal here
Read more about the 4th metacarpal here
Read more about the 5th metacarpal here
Proximal phalanx
Osteologic features of the phalanx:
-
Base -
Shaft -
Head (Proximal and middle phalanx only) -
Tuberosity (Distal phalanx only)
Rays of the Hand
1st Ray(Thumb)
2nd Ray (Index)
3rd Ray (Middle)
4th Ray (Ring)
5th Ray (Pinky)
Arches
Similar to the arches of the feet, the hand also has palmar concavity known as “arches”3.
There are 3 arches:
-
Proximal transverse arch : Composed of proximal carpals and forms the carpal tunel3 -
Distal transverse arch -
Longitudinal arch
Proximal Transverse Arch
The proximal transverse arch is composed of the distal row of carpals3. This arch creates space for the carpal tunnel3. The
Proximal Transverse Arch
The
Longitudinal Arch
The longitudinal arch runs proximal to distal and follows the 2nd and 3rd rays3. The proximal end of the longitudinal arch connects to the carpals via the CMC joint3.
Overall Function
The 3 arches are mechanically related to one another3. The 2nd and 3rd rays which follow the longitudinal arch also serve tie the proximal and distal tranverse arches together3.
The 3 arches support and strengthen eachother through interlinking, but a joint disease, such as rheumatoid arthritis weakens one arch, which results in collapse of the other arches3.
Carpometacarpal Joints
The CMC joint is an articulation between the distal carpal row with the bases of the metacarpals3.
Examination
See table 18.2 of Dutton for physical findings on the hand4
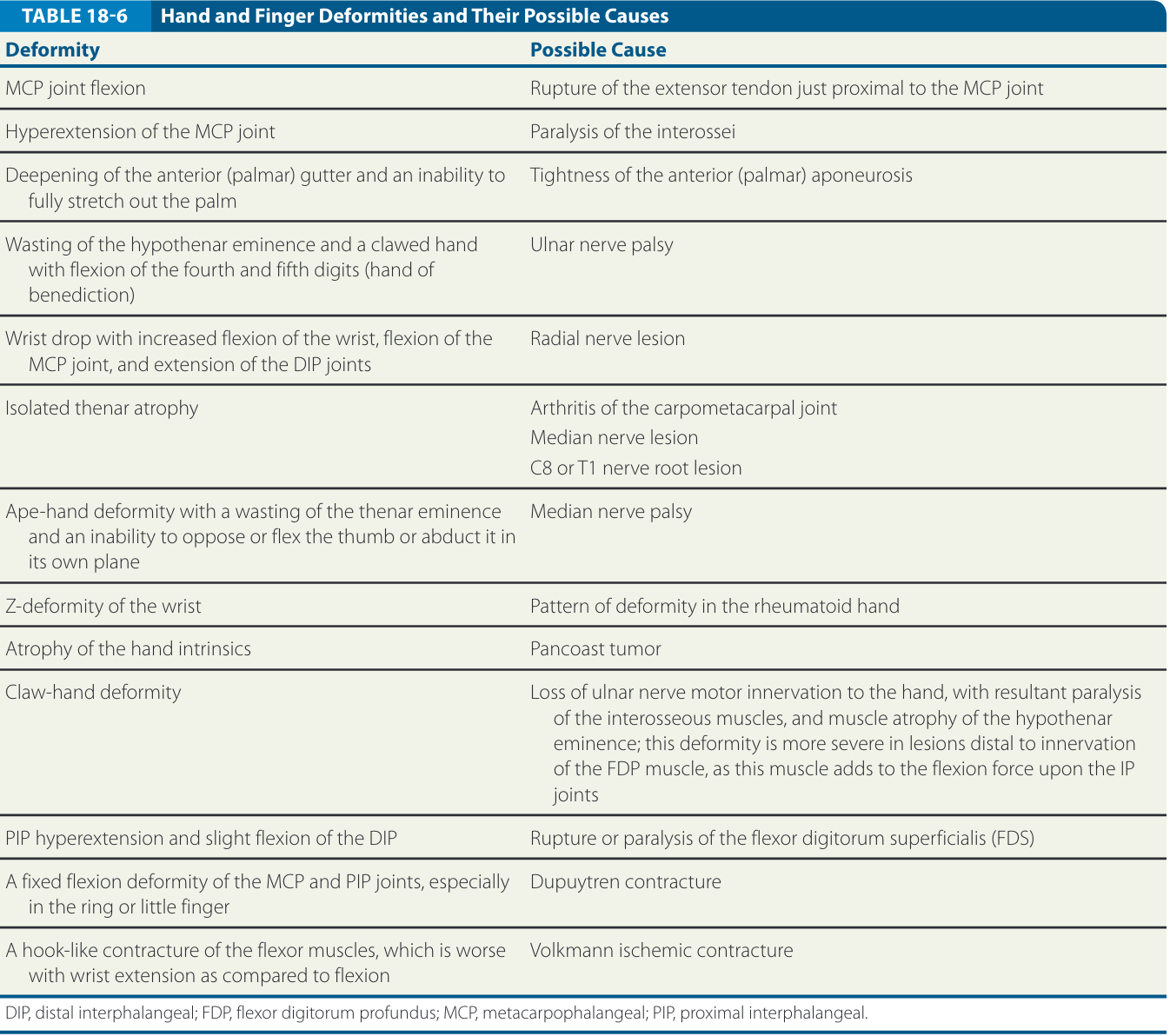
| Deformity | Possible Cause |
|---|---|
| MCP joint flexion | Rupture of extensor tendon just proximal to MCP joint |
| Hyperextension of MCP joint | Interossei paralysis |
| Deepening of anterior (palmar) gutter and inability to fully stretch out the palm | Tightness of anterior aponeurosis |
|
Wasting of hypothenar eminence With clawed hand With flexion of 4-5th digits |
Ulnar nerve palsy |
|
Wrist drop with increased flexion of the wrist Flexion of the MCP joint Extension of the DIP joint |
Radial nerve lesion |
| Isolated thenar atrophy |
Arthritis of CMC joint Median n lesion C8 or T1 lesion |
| Apehand deformity with wasting of thenar eminence and inability to perform thumb opposition or abduction | Median n. palsy |
| Z-deformity of the wrist | Rheumatoid arthritis |
| Atrophy of hand intrinsics | Pancoast tumor |
| Claw-hand deformity |
Loss of <a href=“/The Archive/Anatomy/Nerves/Upper extremity nerves/ulnar_nerve.html#palsy”>ulnar n. motor innervation to the hand resulting in paralysis of interossei and atrophy of hypothenar eminence. This deformity is more severe when lesions are distal to <a href=“/The Archive/Anatomy/Skeletal Muscles/Upper Limb Muscles/Forearm Anterior Compartment/flexor_digitorum_profundus_FDP.html”>FDP muscle |
| PIP hyperextension and slight flexion of DIP | Rupture or paralysis of FDS |
| Fixed flexion deformity of MCP and PIP joints, particularly the 4th finger | Dupuytren contracture |
| Hook-like contracture of the flexor muscles, which is more evident in wrist extension | Volkmann ischemic contracture |
Special Tests
Provocation Tests
Tendon special tests
- The Integrity of the Central Slip (Extensor Hood Rupture): “The patient flexes the finger to 90 degrees at the PIP joint over the edge of the table. The patient is then asked to extend the PIP joint, while the clinician palpates the middle phalanx (Fig. 18-57). The absence of extension force at the PIP joint and fixed extension at the distal joint indicates complete rupture of the central slip. No diagnostic accuracy”4
Ligament Special Tests
Neurovascular Special Teests
Pathologies
- Gamekeeper’s Thumb (Skier’s Thumb) pathology
Manual Therapy
- Pisiform opposition mobilization
Exercises
- Wrist CARs
- Hand tendon gliding
- Pronation
- Supination d
- Wrist ISOs