Tone Management
Spasticity and Rigidity
Muscle Tone
Tone: refers to a relaxed muscle’s resistance to passive stretch/tension
The muscle resists the stretch through both active and passive mechanisms
Passive component
The passive mechanisms refer to viscoelastic structures that are non-contractile.
- Actin & Myosin
- Connective tissue
- etc
Note
Forces created through passive mechanisms are invisible to EMGs
Active component
The active mechanisms refer to contractile motor units
These are controlled by spinal and supraspinal mechanisms
Note
Forces created through active mechanisms can be measured by EMGs
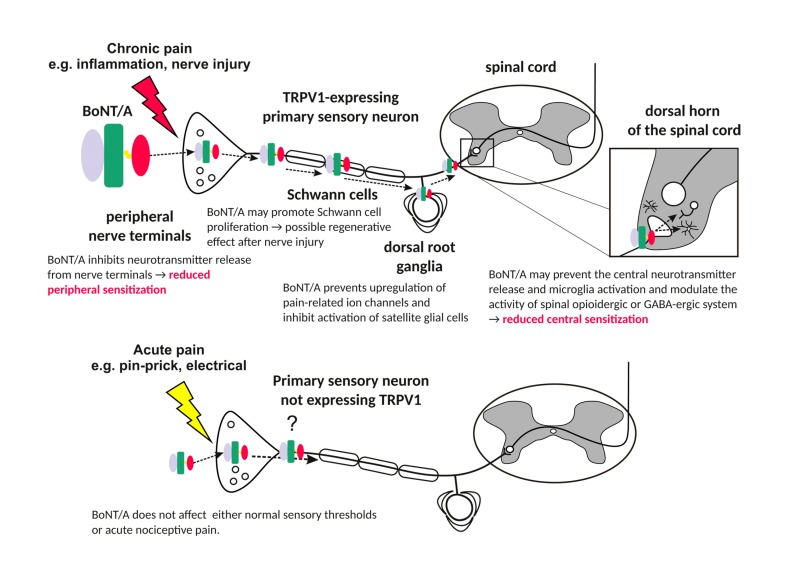
Anatomy
Muscle spindle: Intrafusal fibers
Muscle belly: Extrafusal fibers
Tendon: Connective tissue connecting muscle to bone
Intrafusal Fibers
- “Muscle spindle”
- Sensory organs
- Detects changes in Length AND Velocity
Intrafusal fibers
- Length + velocity
- Ia Afferents → SC
- Length
- Ia and II Afferents → SC
Extrafusal Fibers
- “Muscle belly”
- Contraction creates force and movement
Tendon
- Connects muscle to bone
Both Synapse onto γ-motor neurons in Spinal Cord
Extrafusal fibers
- Contracts muscle itself
- Activated by Alpha Motor Neurons from SC
Stretch Reflexes
Stretch Reflex: ?var:ref-stretch-reflex.definition
Muscle spindles generate tone via the stretch reflex (dynamic or static):
2 types
Dynamic: sudden rapid stretch of a muscle → Ia → SC → alpha motor neuron causes sudden contraction of muscle
Static: Sustained stretch → type II → spinal cord → alpha motor efferents → cause asynchronous contraction of muscle fibers (motor units not all discharging together) = mild sustained contraction of these fibers as long as it is stretched.
This is the physiological basis of maintaining muscle tone
Mechanism
Muscle Stretches → Sensory info send to spinal cord → Muscle contracts to prevent overstretch damage
- Muscle stretches
- Intrafusal fibers sense stretch
- Ia + II afferents send signals to SC
- Synapses onto agonist Alpha motor efferents
- Agonist muscle contracts
Patellar Tendon Reflex
Alpha motor neurons → Extrafusal fiber contracts to prevent overstretching Quadriceps contract
Reciprocal Inhibition
Within spinal cord, Ia & II afferents also synapse onto:
- Inhibitory Interneurons of alpha motor neurons
- Inhibits alpha motor neurons of antagonist muscles while agonist contracts
Result: Antagonist muscle cannot contract preventing further stretch of the agonist
How Do They work during muscle stretch
Patellar Tendon Reflex
- Hammer hit at tendon
- Quadricep muscle is stretched → Stretching both the intrafusal and extrafusal fibers
- Intrafusal fibers detect stretch (length/velocity)
- Type Ia and II afferent fibers
- Signals carried to DRG
- To dorsal horn of spinal cord and synapses on:
From dorsal horn to α-efferent
- Motor neuron (alpha/efferent)
- quad extrafusal fiber and cause it to contract to protect the muscle from overstretching (a monosynaptic reflex)
From dorsal horn to interneuron
- Interneuron → reciprocal inhibition
- Reciprocal inhibition
- inhibits alpha-motor efferents of antagonist muscles (Hamstrings relax)
Recurrent inhibition
- Motor neuron fires → activates inhibitory interneuron
- Inhibits the same neuron or a group of neurons.
- Mediated by Renshaw cells in spinal cord
This feedback loop helps regulate motor neuron activity, preventing excessive firing and contributing to the fine-tuning of motor control.
Found to be increased in those with SCI - Overexcitation1.
Important
VERY DEBATED IF INVOLVED IN SPASTICITY
Alpha-Gamma (α-γ) Coactivation
Alpha-Gamma (α-γ) Coactivation: ?var:ref-alpha-gamma-coactivation.definition
Body needs to maintain stretch sensation when a muscle is contracting:
- Muscle contraction
- Extrafusal fibers and intrafusal fibers contract
- Muscle spindle tension is maintained due to the intrafusal fiber contraction
- Maintains the firing rate of type Ia fibers in an optimal range for detecting a change in muscle length
Tip
HYPOTHETICALLY if ONLY alpha-motor efferents are excited and Extrafusal fibers contract → reduces tension on muscle spindle → desensitization → decreased stretch proprioception info
HOWEVER this is not exactly what happens because the body needs to have stretch sensation during contraction/shortening!
Summary
- Muscle stretches
- Intrafusal fibers sense stretch
- Ia + II afferents send signals to SC
- Synapses onto agonist α-motor efferents
- Synapses onto inhibitory interneurons
- Synapse on Agonist gamma-motor efferent
- Stimulates agonist intrafusal fiber contraction → tensioning muscle spindle to maintain stretch sensitization
- Synapse on Inhibitory Interneuron of antagonist gamma-motor efferent
- Inhibits gamma motor neuron to antagonist muscle, decreasing tension on antagonist muscle spindle (desensitized to stretch)
Intrafusal and Extrafusal fibers’ role in proprioception
To provide proprioception, the intrafusal fibers must contract and stretch in parallel with the extrafusal fibers MM Stretch → both intrafusal and extrafusal are stretched → type Ia/II → sensitive to stretch During a stretch, the stretch on the intrafusal fibers provide proprioceptive information of a muscle stretch MM Contraction → you would expect extrafusal contraction and intrafusal fibers to not contract However, not exactly the case;alpha gamma co-activation Alpha and gamma motor neurons contract in parallel in order to maintain tension on the intrafusal sensory fibers to provide proprioception during contraction
GTOS: Prevents tendon avulsion
Golgi tendon organs (GTOs) are sensory organs found within tendons
These organs detect tendon stretch and send sensory signals via Type 1b afferents → spinal cord.
GTO Example: Ego bicep curling
Muscle contraction → tendon lengthens → GTOs are proprioceptive/sense length → type 1b afferents → SC → DRG → synapses onto 2 interneurons:
Inhibitory interneuron
The inhibitory interneuron is activated which inhibits the alpha motor neuron to the bicep → Decreasing tension of agonist (bicep)
Excitatory Interneuron
Antagonist contraction to pull forearm in opposite direction Interneuron → alpha motor neuron → Excites antagonist (triceps)
Questions?
Supraspinal influences
CST and RST tracts
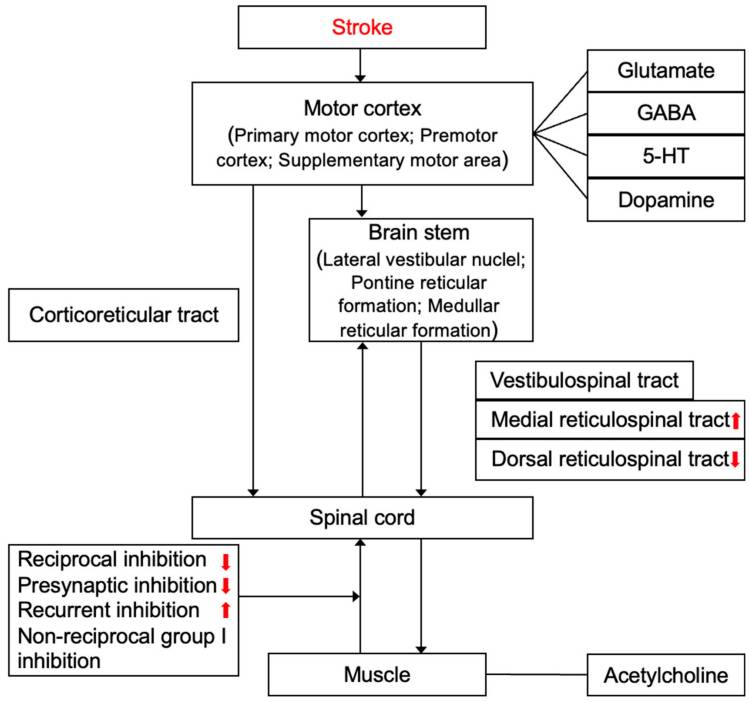
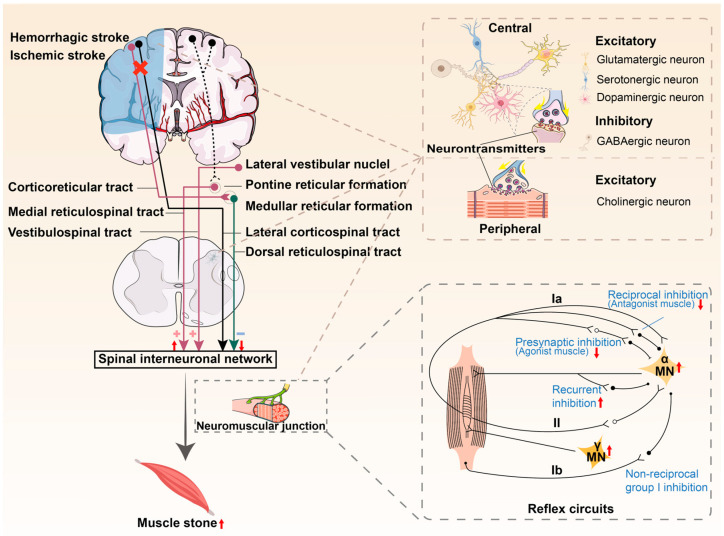
Corticospinal Tract
- Cerebral cortex → crosses at pyramidal decussation → motor neurons
- Inhibits lower motor neurons
- Gives off corticoreticular pathway on way down → medullary reticulospinal nuclei → reticulospinal (RST) tract
- Inhibits lower motor neurons
see image on slide18
slide 19
- Supraspinal: facilitatory and inhibitory long tracts + cerebellum,BG, limbic system and more thought to modulate muscle tone…
- Inhibitory: All work to reduce excitability of motor neurons/dec muscle tone:
- CST: inhibits spinal reflexes, helping with fine tuning of motor commands, suppressing excessive reflex activity. Crucial for voluntary motor control
- Dorsal RST: suppresses muscle tone, usually during REM sleep or motor control tasks
- Facilitatory: All work to increase excitability of motor neurons, increasing tone
- VST: tonic drive reflects motion and position of head and projects to extensor muscles, provides drive to facilitate antigravity support. Disruption leads to dec’d extensor tone/postural instability
- Medial RST: excites motor neurons controlling axial/proximal limb muscles, supporting postural adjustments/locomotion
Hypertonia/ Hyperreflexia in UMN Lesions
Where does it all go wrong?
UMN Lesion → Hypertonia/Reflexia
Damage in Cerebrum:
- Inhibition of medullary RST/CST → Disinhibition of motor neurons:
- Increase alpha motor excitation → inc in extrafusal fiber contraction → HYPERTONIA
- Increase gamma motor excitation → inc in intrafusal fiber contraction → sensitized intrafusal fibers → reflex pathway activates → HYPERREFLEXIA
slide 22
MANY pathways are involved… medullary RST has a large effect on Hypertonia/Hyperreflexia
Studies show later on RST may take over more muscle mvmt to make up for dysfunctional CST in Spasticity (Sangari et al, 2019)
Clonus
Pathological reduction in Reciprocal inhibition due to supraspinal lesions, leading to contract-relax cycles as muscles are stretched/contracted.
Spasms
This heightened reflex activity can result in involuntary muscle spasms, which are sudden, often painful contractions of the muscle in response to stretch
Spasticity & Rigidity
| Differentiating Points | Spasticity | Rigidity |
|---|---|---|
| Velocity dependency | Yes | No |
| Resistance to movement | In one direction (flexion or extension) | In both directions |
| Length dependency | Yes | No |
| Type of hypertonicity | Clasp-knife | Lead pipe or Cog-wheel |
Clasp Knife Effect
- High velocity of quick stretch activates nuclear bag then Ia afferents → sudden contraction
- Further into the stretch, the stretch is detected further by nuclear bag and nuclear chain fibers → Ia and II afferents activate → α-motor neuron → contract → maintains the resistance through some of the range
- Release: Golgi tendon organ (Ib afferent) activate, which inhibits α-motor neurons, reducing resistance, allowing some stretch. → like a tardieu 2 - catch + release
| Grade | Criteria |
|---|---|
| 0 | No resistance throughout the course of the passive movement |
| 1 | Slight resistance throughout the course of the passive movement, followed by release |
| 2 | Clear catch at precise angle, interrupting the passive movement, followed by release |
| 3 | Fatigable clonus <10 seconds when maintaining pressure occurring at precise angle |
| 4 | Infatigable clonus >10 seconds when maintaining pressure occurring at precise angle |
Why are only some muscles spastic?
- More Excitable To Begin With
- Biceps, PFs are more excitable/experience more spasticity because they are more used throughout our daily life
- Excitability amplified after injury
Synergies + Spasticity
Why do we have them?
- Error compensation - if one muscle is weak, others help achieve motion
- Energy efficiency- CNS reduces complexity of mvmt by organizing muscles into synergies, allows for quick/automatic mvmts without higher level control
- UE: flexor synergy dominant
- LE: extensor synergy dominant
Synergies
After UMN lesion
- CST is damaged, body increases reliance on RST - less capable of fine motor, better at gross motor control - leading to synergistic mvmts
- RST Is disinhibited (excited), causing involuntary co contraction – ie trying to lift shoulder, elbow + wrist flex too
MMTs are not indicated for Synergistic Muscles
Synergies make MMTs inaccurate
Co-activation of other muscles makes it impossible to isolate 1 muscle
Not purely volitional movement, but rather more automatic driven (RST)Mooney2024?
Instead- staging with Brunnstrom post stroke can be helpful
Benefits of Spasticity
- Can improve functional activities like transfers, standing, gripping
- Acute increases can also be a sign: UTI, fracture, pressure sore
- Improves venous return/circulation
- Protects against DVTs
- Reduces fracture risk, decreases risk of osteoporosis
- Protects against muscle atrophy
- Marker of motor recovery potential
However spasticity can interfere with functional activities which is when intervention is indicated…
Tonic & Phasic Spasticity
- Velocity dependent increase in tonic stretch reflex (tone), hyperexcitability of stretch reflex
- Spasticity can be “phasic” or “tonic” d/t predominant involvement of different components of stretch reflex.
- Phasic involuntary mm contraction after quick stretch, clonus. Hyperactive phasic stretch reflex
- Tonic (static): hyperactive tonic stretch reflex seen in chronic spasticity/non ambulatory pts, passive stretch at ankle (experts argue this is just rigidity/severe hypertonia rather than true spasticity)
- Happens after spasticity affects patient over time
| Feature | Phasic Spasticity | Tonic Spasticity |
|---|---|---|
| Trigger | Rapid stretch | Sustained posturing |
| Velocity-Dependent | Yes | No |
| Neural Mechanism | Exaggerated stretch reflex (Ia afferents) → activates alpha motor neurons | Continuous excitation of α- and γ-motor neurons from Ia and II afferents |
| Clinical Sign | Clonus, quick spasms | Constant stiffness, resistance to movement |
Pathophysiology
Spasticity is mostly due to dis-inhibition of the medullary (dorsal) Reticulospinal tract
- Spasticity may be maintained through facilitatory influences of the medial (pontine) RST
- Vestibulospinal tract plays a minor role
- As shown by sectioning studies of the human spinal cord in those w/ spasticity
- Other brain regions may also be involved: BG, cerebellum, etc
- Studies are still examining all influences on spasticity/tone – a lot is still unknown…
Spinal Influence/SCI spasticity
Spinal influence:
Many different ways to inc excitation or dec inhibition in spinal cord
Descending monoaminergic drive normally excites alpha motor neurons and inhibits dorsal horn/sensory input
SCI Chronicity
Acute stage of SCI: loss of monoaminergic influence → causes hypo excitability of motor neurons and excitation of sensory input
Chronic SCI Spasticity →Product of overactive motor neurons Weeks after disconnection from supraspinal input, motor neurons transition into an excitable state, really responsive to excitatory NTs like glutamate. Leads to muscle contractions, easily triggered by touch/mm stretching.
SCI SEVERITY
Incomplete SCI
Incomplete/partial myelopathy involving lateral funiculus: If there is involvement of CST only, it will result in weakness, hypotonia and loss of superficial reflexes. If there is additional involvement of dorsal RST, spasticity and hyperreflexia will develop due to unopposed activity of medial RST. Spasticity will be predominant in antigravity muscles and will result in paraplegia in extension and extensor spasms. Flexor spasms can occur if FRA are activated by pressure sores.
On the other hand, if there is involvement of dorsal RST only with sparing CST, there will be spasticity without much weakness.
Complete SCI
Complete myelopathy with involvement of all four tracts: Spasticity will be less in this case because of lack of facilitatory input from medial RST and VST. Disinhibition of FRA will result in paraplegia in flexion and flexor spasms.
Parkinsonian Rigidity
Rigidity: Increased resistance to passive movement, affecting both flexor and extensor muscles in Parkinson’s disease
Neural mechanisms are incompletely understood
Types of Rigidity
Lead-pipe rigidity: a uniform, constant resistance throughout the range of motion, typically seen in conditions like Parkinson’s disease.
Cogwheel rigidity: involves intermittent jerks during movement due to oscillations between the agonist and antagonist muscles.
| Cogwheel | Leadpipe |
|---|---|
| Rigidity + tremor | Smooth, consistent |
| Tonic increase in muscle tone2 | EMG studies show phasic bursts of muscle activity3 |
Can be an underlying tremor that is not overtly present yet
Asci F, Falletti M, Zampogna A, et al. Rigidity in Parkinson’s disease: evidence from biomechanical and neurophysiological measures. Brain. 2023;146(9):3705-3718. doi:10.1093/brain/awad114
Pathomechanism
The direct pathway normally facilitates movement by disinhibiting (EXCITES) the motor cortex.
The indirect pathway inhibits movement:
- Becomes overactive (due to lack of dopamine) in PD
- Increases inhibition of the motor cortex
- Dec activation of CST/RST
- Causes inc activation of alpha motor neurons → Rigidity/bradykinesia.
Rigidity
Rigidity is end-stage form of this neurophysiological process
- Basal ganglia increase inhibitory output
- Excessive α-motor neurons
- Sustained muscle contraction (Rigidity)
Other potential mechanisms
- Exaggeration of long-latency stretch reflexes (LLSR)
- Enhanced shortening reaction (SR) and stretch-induced inhibition (SII)
- Involvement of brainstem circuits involving sublaterodorsal nucleus, nucleus reticularis gigantocellularis (NRGC), locus coeruleus, caudal raphe and pedunculopontine nucleus (PPN)
- Alteration in functional connectivity in brain networks involving frontoparietal connection, premotor-pre-cuneus connection
- Non-neural factors like viscoelastic properties of muscle fiber and surrounding connective tissues
Tremor
Pathomechanism
Involved in other paths within the basal ganglia-thalamo-cortico loop:
BG inhibits thalamus → causing altered firing patterns generating rhythmic bursting activity of thalamic cells
Spasticity Management
As based on AAPM&R Consensus Guidelines 2024
Surgical Treatments
Selective Dorsal Rhizotomy (A)
Selective Dorsal Rhizotomy: Irreversible surgery where a surgeon cuts sensory neurons in order to prevents stretch reflex/afferents from contributing spasticity
- Primarily for children 4-10 years old or some adults with CP who are unresponsive to other treatments
- Diffuse Spasticity
- Decreases spasticity as far as 17 years after surgery
- After SDR, early intense PT is indicated to capitalize on opportunities to change motor patterning
- Monitor for Dysesthesias: Gabapentin given if experienced, usually lasts a couple of weeks
Criteria
Usual Criteria:
- Prematurity,
- Diplegia CP,
- GMFCS I-III,
- Age 4-10 y/o,
- Pure spasticity
- Antigravity hip flexor strength,
- Adequate cognition,
- Absence of contractures,
- Periventricular leukomalacia with no basal ganglia or thalamic lesions on imaging
Following surgery, changes in tone creates opportunities to change motor patterning. Initial intense PT rec: Early aggressive OP PT 2x per week or 6 weeks of intensive inpatient PT
Other Considerations
- Dec spasticity as far as 17 years after surgery
- Deep tendon reflexes and clonus is absent after
- Absence of patellar reflex can lead to patients having an inc in falls from inadvertent knee flexion in stance bc of the absence of normal knee extension reflex when knee is suddenly flexed. Pts adapt over time to this change.
- Safe procedure, long term complications rare - some side effects include dysesthesias, urinary retention, numbness, infections and cerebral spinal leak (<10% of patients)
- Dysesthesia risk inc with # rootlets dissected, usually lasts a couple weeks and responds to gabapentin. Nocturnal leg spasms can occur but respond to diazepam.
- Following SDR, recommendations are for patients with knee flexion contractures to wear immobilizers at night thru adolescent growth spurt.
Tendon Lengthening Surgery
- Cutting part/all of tendon to lengthen it
- Typically CP kids, sometimes DMD/SCI/Stroke
- All other options must be trialed prior
Achilles tendon Lengthening
- Indicated with severe contractures
- Usually ≥20° of PF
- Cast 6-12 weeks, crutches 4-6 weeks
- Intensive PT after: Stretches, strengthening and non-articulating AFOs for walking is indicatedGalletti2024?
Warning
Over Lengthening →Worsens gait →Poor power in toe off/risk of crouching in midstance
Neurotomy
Neurotomy: Cutting peripheral motor nerve
Diminishing reflex arc → Reducing spasticity
Mainly for Focal spasticity MAS > 3 (passive mvmt difficult) Indicated after botox is trialed/failed or is too costly 80-85% success rate for dec spasticity
Procedure may induce paralysis or dec strength, but pt can recover strength via other motor nerves helping to compensate
Other Surgeries
Non selective ventral dorsal rhizotomy: children w GMFCS IV or V with sig hypertonia affecting comfort, care, positioning - Both sensory and motor rootlets cut from L1-S2 in nonselective fashion (50-80%) - By preserving a portion of the ventral rootlets, sufficient motor control preserved for some voluntary movements. - Reduction in spasticity/dystonia but some dystonia can return 1-2 years later - However, can significantly weaken legs – reduce standing ability
Note
Selective peripheral - 61-91 % pt satisfaction rate
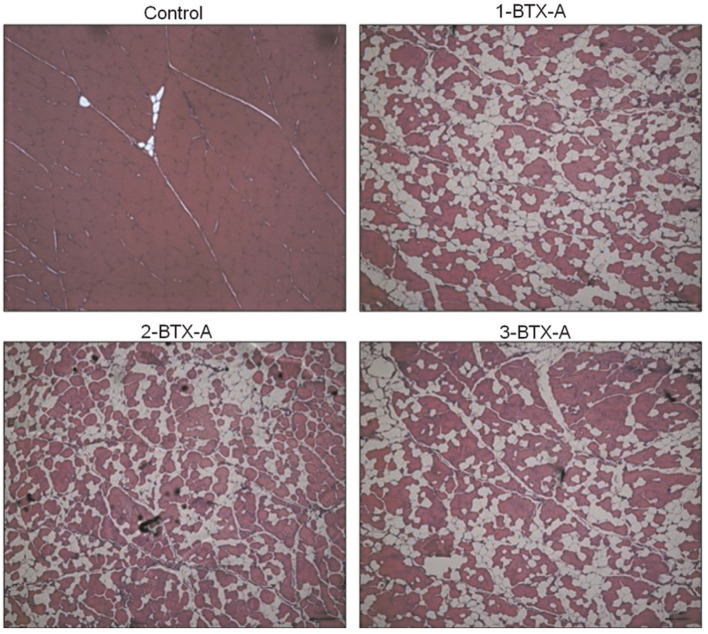
Botox (A)
INJ-1: The AAPM&R Spasticity TEP recommends clinicians consider use of botulinum toxin A for management of focal upper and lower limb spasticity.
- Distal muscles, focal relief
- Inhibits release of Ach
- MAS scores improve
- Effects last 3-4 months
- Peak effect: 3-4 weeks post injectionchen2020?
- May use AFOs/Orthoses post procedure
- Can decrease pain d/t spasticitywissel2016?
- MS, stroke populations
- Problems: expensive, not always covered by Insurance
- Adverse local effects: weakness, pain, leg cramps, skin rash, infection,
- Adverse systemic effects can occur: dysphagia, dysphonia, weakness, dyspnea, respiratory distress
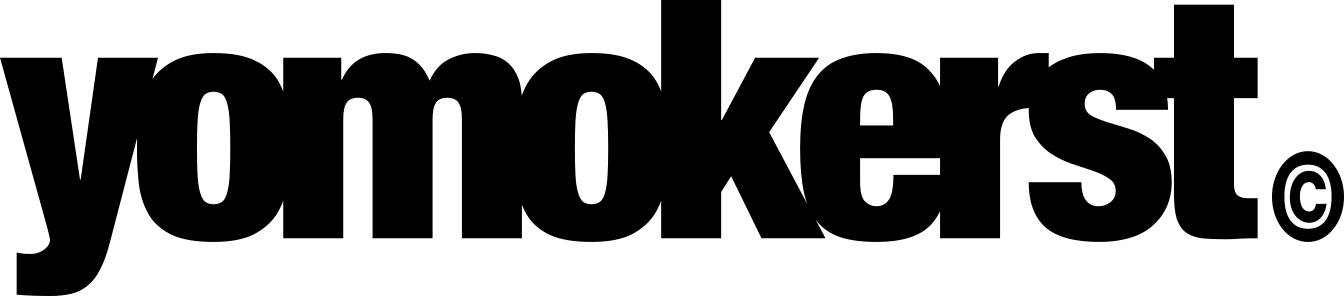
Post-Botox
Reduced muscle size, Fat infiltration, Dec in strength
Animals: after botox = smaller muscle size, strength and more fat infiltration. Muscle strength also reduced in adjacent and contralateral non target muscles.
Humans: a single dose of BoNT has been shown to reduce muscle size in humans for up to 1 year and 50% dec in strength.schroeder2009?
Humans post Stroke: Botox reduces MAS and elbow flexor strength 3 weeks following botox injection.chen2020?
Human histological studieshoward2021? 15 children w/ spastic diplegic CP - botox to gastroc: Measured calf volume: 5% dec in gastroc volume 5 weeks post injection but 4% inc in soleus volume suggesting adjacent muscle hypertrophy to compensate for injected muscle. Study 2: Ultrasound to gastroc: demo’d dec’d volume in children with CP post BoNT injection.
Takeaway
Weigh benefits of decreasing spasticity to cons of decreasing strength when making recommendations
Emphasize strengthening prior/after botox injections in the muscle injected!
3-4 week mark = peak effects: Capitalize on motor patterning!
Can be beneficial for decreasing pain!
Monitor for systemic muscle weakness in those getting recurrent botox injections or high doses- potential side effect
Phenol or Alcohol Blocks ()
INJ-2: The AAPM&R Spasticity TEP suggests that clinicians consider use of phenol or alcohol blocks for management of focal spasticity.
Mild/no sedation.
Target nerve found via estim/ultrasound. Local anesthetic applied, Nerve stimulation performed to find right motor response. Phenol/alcohol then injected, immediately ceasing contractions/spasticity. Chemical denatures protein resulting in neuropraxic injury/denervation
Can lead to wallerian degeneration of targeted nerve
Can also result in fibrosis/local vascular injury/ muscle necrosis due to non-specific protein denaturation
Average duration of effects last 3-9 months (LONGER than botox)
Applied to isolated motor nerves/motor branches Not sensory-would result in painful dysesthesias
NO large scale clinical studies - only small retrospective, case series/case studies: typically a therapy of last resort and reserved for END STAGE THERAPY Stroke, SCI, TBI, CP
Inferior effects compared to botox on spasticity (Gonnade, 2017)
Adverse effects: phenol spreading to adjacent nerves or sensory fibers: Painful dysesthesias range between 10-30% depending on study
Takeaways
Phenol/alcohol injected into motor nerves, immediately ceasing contractions/spasticity. Chemical denatures protein resulting in neuropraxic injury/denervation Average duration of effects last 3-9 months (longer than botox) Usually a tx of last resort- Inferior effects compared to botox on spasticity (Gonnade, 2017) Adverse effects: phenol spreading to sensory fibers: Painful dysesthesias range between 10-30% depending on study
Oral Medications (C)
Pharm-1: The AAPM&R Spasticity TEP suggests use of oral medications to manage generalized or systemic spasticity; oral medications can be used either exclusively or as a component of a multimodal treatment approach.
- No medication is uniformly useful in tx of hypertonia
- All drugs can have serious side effects - negative effects will be weighed when prescribed
Baclofen (C)
- Muscle relaxant
- Most common drug for spasticity of spinal region (ie SCI, MS)
- Can be used in supraspinal spasticity (CP, Stroke)
Some caution w/ use in cerebral forms of spasticity d/t interference with attention/memory on brain injured patients
GABAB Agonist - mainly acts at the spinal level Inhibits excitation of alpha motor neurons
Peak concentrations: 2-3 hrs after ingestion Short half life of 2-6 hours - taken in smaller doses throughout day Adverse effects: weakness, sedation/drowsiness, fatigue, dizziness, constipation, confusion, hypotonia, ataxia. Sudden withdrawal can cause seizures/hallucinationsghanavatian2024?
Baclofen Pump (A)
Baclofen Pump: Pump implanted under the skin of abdomen, then a catheter is then threaded from the pump to spinal fluid in low back, bypassing BBB.
SUR-1: The AAPM&R Spasticity TEP recommends use of intrathecal baclofen pump therapy (ITB) as an effective treatment of spinal or cerebral origin spasticity in appropriately identified patients.
Continuous delivery of baclofen, lower doses compared to oral administration.
Need to trial oral baclofen prior Checking for side effects
Contraindications: infection, insufficient body mass for pump bulk,
- For SEVERE spasticity, when oral meds fail
- Wait ≥1 year after brain/SCI before consideration.
- Global OR regional spasticity for CP, brain injury, stroke, SCI, MS.
- Negative effects on arousal/cognition
- Most meds will last 2-3 months before requiring refill
- Battery lasts 4-7 yrs -need another surgery to replace
Tizanidine
- α-2 adrenergic agonist
- Causes decrease in presynaptic activity of excitatory interneurons in spinal cord
- Decreases stretch reflex activity/motor neuron excitability
Used in Cerebral + Spinal disorders: MS, Stroke, ALS
Sedation, dizziness, dry mouth common after → weakness is not a big problem Lasts 3-6 hours, max effects at 1-2 hours after administration Shown to have a more favorable tolerability profile, less reported mm weakness + less sedation compared to baclofen
Dantrolene
- Acts outside the CNS → muscle fiber level Inhibits release of Ca2+ from Endoplasmic Reticulum in muscle cells
- Ca2+ normally binds onto troponin in actin filaments allowing actin-myosin cross bridging (so inhibiting this decreases contractility of muscles)
- Peak Effects: 1-3.5 hrs after ingestion
- Long lasting: 8-10 hours
Side effects: weakness ( ie respiratory muscle weakness), sedation, GI sx, dizziness, fatigue Big warning for Serious hepatotoxicity Will need to liver eval prior and monitoring after Used for stroke, SCI, CP, MS, etc NOT in ALS- can progress mm weakness Less sedative than baclofen - more preserved cognitive function
Diazepam
- GABAA agonist, acts on Brain + SC (Stroke, CP, TBI)
- Commonly short term only
- Onset of action: 15-60 min
- Duration of onset: 12+ hrs, very long lasting
Side effects:
- Sedation
- Impaired memory/cognition
- Ataxia
- Fatigue
- Confusion
- Depression
- Respiratory depression
- Bradycardia
- Suicidality
- Syncope
- Hypotension
Diazepam Takeaway
- Schedule IV controlled substance w/ potential for abuse
- Abrupt cessation: seizures, hallucinations
- Elderly pts have dec’d renal fxn - not recommended d/t issues w diazepam accumulation/renal issues
Gabapentin
- Inhibits glutamate, creating inhibitory effect for motor neurons
- Usually MS/SCI populations
- Used when other first line drug tx do not work
- Few sedative effects
- Helpful to dec neuropathic pain as well
Cannabinoids/THC
Enhances GABA, reduces effects of Glu New area of research, mostly studied in MS Reduces excitatory neurotransmission → decreasing spasticity Can help tx pain associated w/ spasticity too Moderately effective in reducing spasticity scores, but almost as effective as other drug tx: baclofen, tizanidine (Jones et al, 2020)
Oral Meds Takeaways
Yes: Pain, Interference with ADLs/PT
No: Not for FOCAL spasticity d/t global effects of drugs If spasticity helps w/ walking/functional tasks don’t recommend Weigh other pros of spasticity: DVT prevention, dec risk of osteoporosis, protective marker if something is awry in body
Big risk for adverse effects on cognition/sedation - be sure to educate patients about this when suggesting drugs
Note
In many stroke pts, spasticity is local (1-2 muscle groups) which is easily targeted with Botox or peripheral nerve blocks NOT drugs (Bakheit, 2012). MS/CP/TBI may be more systemic
Non-pharma treatments (NG)
consideration of use of nonpharmacologic interventions from a range of treatment modalities, in conjunction with other therapeutic options to effect spasticity and facilitate the effects of pharmacologic and procedural interventions on spasticity and to improve function and decrease deleterious effects of contributing conditions.
Note
Can not be graded due to limitations in evidence
NMES
SR+ Meta-Analysisstein2015?
- Decreases spasticity + increase ROM when compared to controls
- Most often Tib Ant or Gastroc + combined w gait training
- Both show improvements in tone/stiffness, however over Tib Ant= better improvements in gait/spasticity (Yang, 2018)
Reciprocal inhibition: Short term - when in use up to 15 min aftermilosevic2019?
NMES Actions
- Agonist Estim-Recurrent inhibition or just muscle fatigue
- Antagonist Estim-Reciprocal inhibition
- Other mechanisms
Note
NMES has the potential to induce neuroplasticity within spinal cord pathsbergquist2011? Suppresses exaggerated excitability
Resistance Training
Spasticity can LEAD to weakness Type II → Type I fibers (Fan et al, 2020) Due to Reduced voluntary motor unit recruitment Relative immobilization/Chronic disuse Causes plastic rearrangements in higher centers that further reduces ability to voluntarily recruit motor units → aggravating spasticity (Gracies et al, 2005) Strength training is inconclusive in decreasing spasticity but important to train to minimize atrophy/improve motor control (Brashear et al, 2016)
Antagonist Strengthening
How? Reciprocal Inhibition: when one muscle contracts, the other stretches/relaxes Theory - no direct evidence for this in strength training
How? Reciprocal Inhibition: when one muscle contracts, the other stretches/relaxes Strengthening the antagonist → inhibitory interneurons in SC → inhibits alpha motor neurons connecting to spastic muscle, allowing stretch Dec’d inhibition compared to controls, but inhibition path still occurs with spastic individuals (Morita, 2006) Antagonist contraction can influence cortical plasticity of agonist (Fang, 2014)
Note
Theory -I could not find any evidence for this in strength training, EMG studies show strength training does not influence thissmania2010?
Weight Bearing
WB provides proprioceptive input Activates joint mechanoreceptors, cutaneous receptors (detecting pressure/stretch vibration) Activates spinal interneurons → dec motor neuron excitability to soleus allowing higher reflex thresholds to allow for walkingnakazawa2004?
Note
Why the patellar reflex is not as intense in standing!
Increases afferent input → reduces hyperactive stretch reflex Studies focus on BWTT, kneeling walking, etc show a decrease in MAS scores/Spasticity/Reflexpeurala2005?
- BWTT reduces the amplitude of soleus max H/M ratio in those with SCI, which is a reflection of reduced motor neuron excitability (less tone/spasticity)trimble2001?
- H/M ratio is commonly used to eval balance between excitatory/inhibitory inputs to motor neuronstrimble2001?
- Spastic Pts: typically inc’d H/M ratio (more motor neuron excitabilty)trimble2001?
BWTT vs tilt tableadams2011?
BWTT: decreased tone, flexor spasms and motor neuron excitabilityadams2011?
WB Regressions
Half kneeling
Can improve dissociation Oppo mvmts and positioning of 2 limbs (one in flexion with other in extension) Quadruped, tall kneeling, modified plantigrade (standing w hands on table), standing6
Quadruped
Particularly in those with extensor spasticity Can help induce flexion of hip/knees, providing prolonged stretch to muscle groups Incorporates reciprocal agonist - antagonist muscle recruitment and motor control Can help reduce spasticity through consistent reciprocal inhibition of hypertonic muscles6
Whole Body Vibration
Whole Body Vibration: ?var:ref-whole-body-vibration.definition
Theory
- Proposed to activate Ia and II afferent fibers, increasing sensory input to CNS → Presynaptic inhibition
Studies
- Mechanism of WBVT has not been fully proven
- REDUCES reflex activity by modulating spinal excitability, enhancing voluntary muscle activationkrause2017?
- Spasticity = muscle overreacts to small stretch loads, so by reducing reflex activity, patient can access voluntary muscle activation (supraspinally) betterkrause2017?
Vibration Also Increases Excitation of Brain
Increases excitability of brain areas involved in movement (primary motor/pre-motor shown in fNIRS, EEG studies ) Promotes neuroplasticity of brain areas that are affected in those w/ spasticitymiyara2020?,lopez2017?
Benefits
- ↓ spasticity (Krause, 2017)krause2017?
- ↑ Strength (in stroke, CP and in elderly healthy adults: MVIC, CSA)machado2010?,pulay2023?,tihanyi2007?
- ↑ blood circulationdionello2017?
- ↑ ROM of knee jointkrause2017?
- Better functional outcomes: TUG, 10 MWTdionello2017?
- Benefits proprioception (shown in a post ACL-R populationmoezy2008? via a joint repositioning test)
Vibration Parameters
WBVT for 10 min at <20Hz frequency improves spasticity in UE + LE
Tip
Lasts about 10 min! Capitalize!
Casting
- Maximal stretch → muscle fatigues then elongates
- Cast is changed every 2 weeks to new lengthened position
- After Botox, casting can help facilitate further spasticity reductionwinstein2017? farag2020?
Serial Casting
Serial Casting: Sequence of casts applied in progressively greater ROM over several weeks to inc ROM
Post Strokewinstein2016? aha?
- Level C evidence for mild to moderate elbow/wrist contractures
Pediatric Cerebral Palsymilne2020?
- Dec’d MAS, inc’d DF ROM, improved gait
TBI
- Grade B for improving PROM or preventing loss of ROM
Cons
- Atrophy
- Skin breakdown
- Pain
- Discomfort
- Affects ADLs/Gait
AFOs
- Prevents contractureweinstein2017?
- Increases DF ROM
- Improved gait mechanics, speed
- Improved spasticity via stretch reflex and MASchen2022?
Night Splints
Wrists night splint
- “Strong evidence wearing a splint all night has no effect in reducing spasticity/contracture”lannin2011?
- AHA states it may prevent contractures but data is conflictingwinstein2016?
Ankle night splints
Wearing a foot splint 12+ hours a day did not affect joint mobility in adults post TBI (Sung et al, 2016)
Combo + botox → best effects on spasticity Alone - very mixed/little evidence (Synnot et al, 2017)
Note: more evidence in CP/Pediatric populations although still inconclusive
Aerobic Training
HIIT increases: BDNF, dopamine, neuroplasticity/retention/learning, attenuates neurodegeneration, helps mood, etc also….
- Changes cortical inhibitionabraha2018?
- Decreases motor neuron excitabilitybulbulian1986?
- H/M ratio after low vs high intensity exercises in a healthy population
Treadmill for 20 min:
- 12.8% reduction in H/M ratio (w/ 40% Vo2)
- 21.5% reduction in H/M ratio (w/ 75% Vo2)
- Decreases Spasticity Acutely in ppl w/ stroke (Sakamoto et al 2014)
- Picture: exercise: 1 arm cycling at 50% max workload for 10 min, control is rest. Measured spasticity in OPPOSITE arm.
- Decreases spasticity in rat model of SCI - through BDNF modulating excitability in spinebeverungen2020?
Stretching
- Not enough evidence for long term spasticity management
- Passive stretches may have SHORT term decreases in spasticity, NOT long termBovendEerdt2008?
- Any effect on motor neuron excitability?
- Mixed resultsBovendEerdt2008?
SR Figure: Non-statistically significant results in favor of the stretching group were observed for MAS, but ROM/functional tasks (ie gait) showed no differencegomez2021?
Could help prevent contractures/dec pain, although no conclusive evidence
Stretch-Contract
Limitations
- Only studies in healthy adults6,fukara2022?
- Likely short term effects (ROM)
- Lengthening a spastic muscle followed by contraciton of antagonist (Induces Reciprocal Inhibition)
- Lengthen spastic mm + contraction of spastic mm (induces Recurrent Inhibition)
Cryotherapy
- Decreases nerve conduction velocity, dec H/M ratioabdelhakiem2024?
- Multiple studies show dec in spasticity post icingabdelhakiem2024?,garcia2019?,alcantara2019?
- 20 minutes of icing → decreased PF spasticity for up to 30 min post icing
- Did not affect proprioceptiongarcia2019?
- No effects on muscle torque capacityalcantara2019?
Thermotherapy
- Can dampen muscle excitability
- Dosage: 10min, 106°F warm foot bath
- Effects: Decreased muscle tone for ≤30minmatsumoto2006?,matsumoto2010?,matsumoto2014?.
Aquatic therapy in warm water can also decrease spasticitykesikatas2004?
Kinesiotape
Wang, 2019 SRwang2019?
KT improved patients’ lower extremity spasticity, motor function, balance, ambulation, gait parameters, and daily activities, with few adverse effects.
Puce et al 2020puce2020?
- Para Athletes w spasticity
- KT decreased the amplitude of stretch reflex (p < .001) compared to placebo
- Strength + MAS did not change after KT, but numeric rating scale scores for spasticity significantly decreased (p = .001).
- Swimming performance was significantly improved after KT treatment as compared with baseline (p < .01)
Inhibitory kinesiotapingmehraein2021? Application of inhibitory KT was found to be able to reduce the Hmax/Mmax ratio in patients with stroke. No sig change in MAS
Limited number of studies, hypothesized d/t recurrent inhibition of hypertonic mm or proprioceptive effects
Deep Pressure to Tendon
Deep pressure to tendon Compressive pressure over longitudinal axis of tendon of a hypertonic muscle to activate GTOs GTOs could help induce elongation to muscle as it feels itself being stretched, thus reducing tone.cite?
Joint Traction
Joint Traction May increase joint awareness w/ inc’d activation of joint receptorscite?
Biofeedback
Children w/ Spastic CP, 10 min a day + visual/auditory signals while pt performed contraction of tib ant and relaxation of tri surae. Significant dec in spasticity (MAS) for up to 3 monthsdursan2004?
PD Rigidity Treatments
Stretches
- Low quality evidence to support
- Many studies show slight dec in rigidity, not to significant levels
Aerobic activity
WBVT - Rigidity scores improve in RCTscite? - 6Hz , amp: 3mmcite?
Botox
- Can dec rigidity scores based on RCTscite?
Pharma
- Big effects on rigidity, high quality evidencecite?
Deep Brain Stimulation
- What? → Surgical treatment using electrical stimulation of brain areas
- Who? → those who have intense symptoms during OFF periods w/ their medications, Used for dystonia, rigidity, tremor
- NOT for those with imbalance issues, memory problems, olderhariz2022?
- Expect → lower med dosages, shorter OFF periods, reduced rigidityhariz2022?,krack2019?,mahlkencht2022?
| DBS site | Effect of therapy |
|---|---|
| Thalamus (Vim) | Reduces tremor but not the other symptoms of PD |
| Globus pallidus (GPi) | Reduces tremor, rigidity, bradykinesia, gait problems, dyskinesia |
| Subthalamic nucleus (STN) | Reduces tremor, rigidity, bradykinesia, gait problems, dyskinesia |
Future Interventions
Conclusion
- Experiment
- Reassess
Reassess
My recommendation for treatment of Spasticity/Hypertonia: Test, retest!
With Tardieu (Spasticity) or MAS (Tone)
Tardieu tests at different velocities - spasticity is velocity dependent so if you use MAS, you may not pick up on spasticity
Summary
Most Common Types of Hypertonia: Rigidity/Spasticity
- Stroke/SCI etc → Spasticity →d/t loss of inhibition from CST/RST/ overexcitation of motor neurons
- PD → Rigidity → BG degeneration
- Many PT treatment options for reductions in spasticity/rigidity → important to test- retest with MAS/Tardieu scales!
Post-Stroke Spasticity
| Spastic muscles | Effect on function | Best treatment option |
|---|---|---|
| Shoulder adductors | Difficult access to axilla for cleaning; difficult to don upper body garments | BoNT into pectoralis major ± subscapularis |
| Elbow flexors | Difficult to reach objects; difficult to don upper body garments | BoNT into biceps brachii and brachioradialis |
| Wrist flexors | Difficult to apply hand splint | BoNT into flexor carpi ulnaris and flexor carpi radialis |
| Finger flexors | Difficult access to palm of hand for cleaning; difficult to access finger nails for cutting; difficult to apply hand splint | BoNT into flexor digitorum sublimis and flexor digitorum profundus |
| Hip adductors | Difficult access to perineal area for cleaning, catheterization, etc. | Obturator nerve block |
| Hamstrings | Knee flexion interfering with gait | BoNT into medial and lateral hamstrings |
| Ankle plantar flexors/invertors | Equinus or equinovarus foot deformity causing tripping and falls | BoNT into gastrocnemius ± tibialis posterior |
| Drug | Effective dose range; maximum daily dose | Most frequently reported adverse effects |
|---|---|---|
| Baclofen | 15–60 mg; maximum 100 mg | Confusion, hallucinations, seizures, fatigue, gastrointestinal symptoms |
| Tizanidine | 6–24 mg; maximum 36 mg | Hypotension, bradycardia, hallucinations, confusion, fatigue |
| Dantrolene | 75–150 mg; maximum 400 mg | Liver dysfunction, dizziness, generalized weakness, gastrointestinal symptoms |
| Diazepam | 15–60 mg; maximum 60 mg | Sedation, amnesia, mental confusion, depression, dependence |
References